
Translate this page into:
Emerging hybrid techniques in aortic valve interventions: A systematic review of integrating surgical and transcatheter approaches
Address for correspondence: Muhammad Ali Muzammil, Department of Internal Medicine, Dow University of Health Sciences, Karachi 74200, Pakistan. E-mail: Muzammil200077@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Qassim Uninversity and was migrated to Scientific Scholar after the change of Publisher.
Abstract
ABSTRACT
Objective:
This systematic review examines the development and clinical application of hybrid aortic valve interventions that integrate surgical and transcatheter techniques. It focuses on the efficacy, outcomes, and innovations of these procedures, particularly for patients at moderate-to-high surgical risk.
Methods:
A comprehensive database search (PubMed, Ovid, Web of Science, Cochrane, CINAHL, Embase, Scopus) was conducted from August 20 to October 10, 2024. Studies on aortic valve interventions combining surgical and transcatheter approaches were included, encompassing case studies, series, cohort studies, and reviews. Non-English articles, gray literature, cadaveric, and animal studies were excluded. Screening followed Preferred Reporting Items for Systematic Review and Meta-Analysis 2023 guidelines, with two rounds performed. Formal quality assessment was omitted due to study heterogeneity.
Results:
Out of 2046 initial articles, 495 unique studies remained after duplicate removal, and 65 articles were selected for analysis. Hybrid aortic valve procedures, blending surgical techniques with transcatheter aortic valve implantation, demonstrated improved outcomes, including shorter recovery times, reduced complications, and personalized treatment options for moderate-risk patients.
Conclusion:
Hybrid aortic valve interventions mark a significant advancement, enhancing patient-specific care and outcomes. Continued innovation in materials, techniques, and clinician training is crucial to improve durability, long-term outcomes, and broader adoption of these minimally invasive procedures. Future research should address these areas to further optimize cardiovascular care.
Keywords
Aortic valve interventions
hybrid techniques
transcatheter approaches

Introduction
Certain aortic valve disorders, such as stenosis and regurgitation, necessitate surgical intervention to correct defective valves.[1] Aortic valve stenosis results from the calcification and degeneration of the valve leaflets, a process associated with aging. Blood flow from the left ventricle to the aorta is restricted as the valve constricts. When the valve undergoes significant constriction, resulting in the occurrence of symptoms such as angina, dyspnea, and syncope, it becomes necessary to intervene.[2] According to the second citation, aortic regurgitation is characterized by inadequate aortic valve closure during diastole, resulting in retrograde blood flow through the aortic valve. Surgical procedures adhere to the 2014 guidelines established by the American Heart Association (AHA)/American College of Cardiology (ACC).[3] Aortic valve failure is treated through a variety of therapeutic interventions. Replacement of the aortic valve is a frequently used treatment for extensive aortic valve disease.[4] The procedure entails the replacement of a dysfunctional valve with either a mechanical or bioprosthetic valve to restore normal blood circulation. Surgical aortic valve replacement (SAVR) is the conventional procedure, whereas transcatheter aortic valve replacement (TAVR) is a less invasive treatment that is ideal for elderly or high-risk patients.[5] Aortic valve repair is a medical procedure used to treat congenital valve defects or particular instances of aortic regurgitation.[6] The goal of this procedure is to preserve the original valve and its physiological function. Procedures involving the aortic valve require a comprehensive strategy incorporating multiple disciplines.[7]
Methods
A systematic review was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. An extensive electronic search was performed from August 20, 2024, to October 10, 2024, in PubMed, Ovid, Web of Science, Cochrane Library, CINAHL, Embase, and Scopus databases, without applying filters for publication status or date. The PRISMA 2023 flow diagram [Figure 1] was used to detail the research selection process. Studies that focused on the use of hybrid techniques for aortic valve interventions, including transcatheter approaches, were selected. Eligible study designs included case studies, case series, cross-sectional studies, case–control studies, cohort studies, and review articles. Only English-language publications were considered, while preprints, non-English articles, and gray literature were excluded. Full-text access limitations, letters to the editor, conference abstracts, systematic reviews, cadaveric, and animal studies were also excluded. The screening process was conducted in two phases: An initial screening of titles and abstracts, followed by a full-text review. All authors participated in the screening and data tabulation, recording their findings in an Excel sheet. Due to the heterogeneity of the topic and the range of study designs, a formal quality assessment was not conducted.
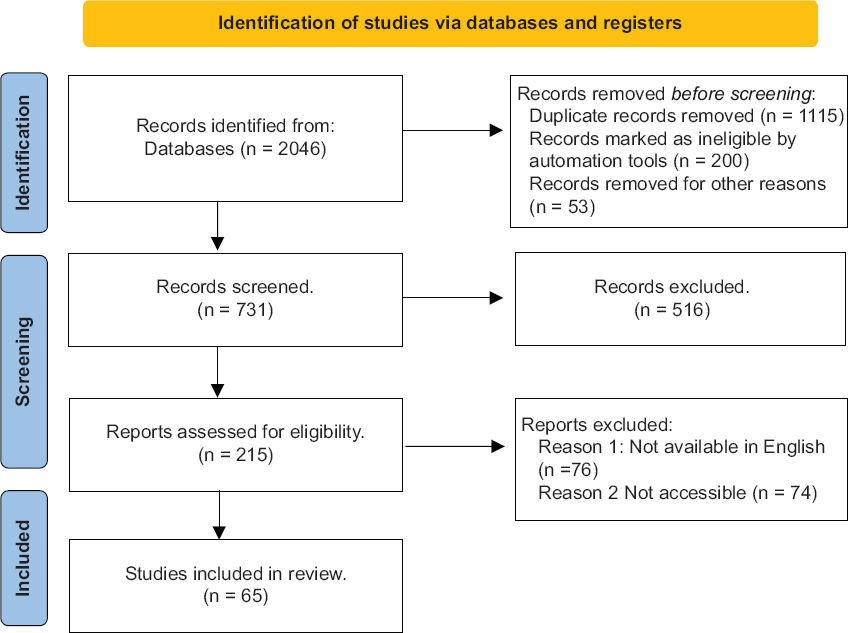
- PRISMA flowchart of included studies
Results
After filtering out duplicates and items that were irrelevant to our research query from the initial database search’s 2046 results, 495 unique articles were found. 65 studies were chosen for additional analysis after the articles underwent two rounds of screening. The PRISMA 2023 flow chart [Figure 1] further explains the procedures and outcomes.
Importance of emerging hybrid techniques
Hybrid techniques for aortic valve interventions have recently emerged rapidly due to their potential to revolutionize aortic valve disease treatment. It employs both surgical and transcatheter techniques. It has numerous benefits, including improved patient outcomes, decreased invasiveness, customized treatments for unique patient characteristics, and expanding treatment options for a broader patient range by expanding eligibility. The field of aortic valve interventions is rapidly progressing, as demonstrated by the continuous technological and procedural breakthroughs observed in the development of TAVR throughout time.[8]
Medical organizations have recognized the importance of hybrid techniques, and updated guidelines are being issued to incorporate them.[9] Insurance coverage and reimbursement policies are also changing to accommodate these new interventions.[10]
TAVR advances
Evolution and refinements in TAVR
TAVR involves replacing a dysfunctional aortic valve without open heart surgery and has seen advancements in various aspects that have improved and revolutionized aortic valve disease treatment over the years. TAVR has undergone continuous technological advancements, including improved valve designs, delivery systems, and imaging techniques, making the procedure safer and more effective.[8]
Initially, TAVR was reserved for high-risk or inoperable patients. However, as clinical trials and research have progressed, its indications have been expanded to include intermediate-risk patients, broadening the population that can benefit from this minimally invasive procedure.[11] Furthermore, ongoing research has contributed to decreased complications, improved patient outcomes, and a higher safety profile, resulting in TAVR being accepted as a standard of care for aortic stenosis in many cases.[12] There have also been reports of faster recovery and shorter hospital stays due to procedural refinements.[13] The Centers for Medicare and Medicaid Services has recognized the importance of TAVR and has expanded its coverage, ensuring improved accessibility to this therapeutic intervention.[14]
As the field of TAVR progresses from a research-based intervention to a widely accepted therapeutic approach for aortic valve pathology, increased scholarly investigation and technological advancements will further improve this area, providing additional benefits to individuals requiring aortic valve replacement.
A comparison of TAVR with traditional surgical options
A comprehensive analysis of TAVR about conventional surgical alternatives, particularly SAVR, can yield significant insights regarding the advantages and effectiveness of these interventions. Both approaches possess unique advantages and disadvantages; so, the ultimate decision relies on the specific circumstances of the patient.
TAVR is performed through a small incision to ensure minimal invasion and less trauma to the patient.[14] Meanwhile, SAVR is a more invasive open-heart surgery that requires a sternotomy (splitting the breastbone).[15] Furthermore, as a result of its restricted invasiveness and diminished stress, TAVR is linked to a shorter recovery period, shortened hospital stay, and accelerated return to normal activities.[16] The SAVR operation is linked with a prolonged period of recovery and hospital stay, as well as a significant delay in returning to normal activities.[17] Furthermore, it is important to acknowledge that the utilization of TAVR was initially limited to individuals who were classified as high-risk or ineligible for conventional surgical procedures. Nevertheless, there has been a recent extension in its utilization to include individuals with moderate risk as well.[18]
SAVR treats a broader range of patients than TAVR, including those with complex valve issues.[17] The superior long-term outcomes of TAVR over SAVR in terms of survival make it a better option for high-risk patients.[18] As previously stated, TAVR results in a shorter hospital stay, demonstrating its cost-effectiveness in some studies.[19,20] However, in the long run, SAVR may be more cost-effective for low-risk patients.[17] There are several TAVR access points, including transfemoral, transapical, and transaortic.[15] SAVR, on the other hand, requires traditional open-chest access.
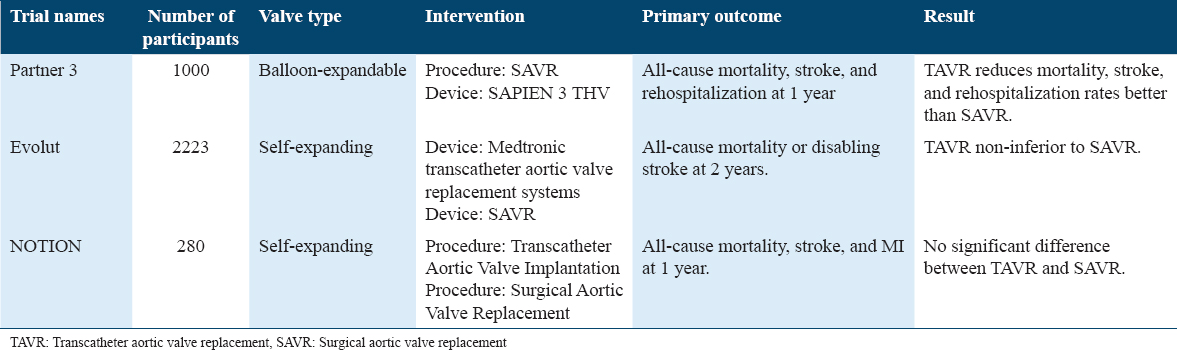
Table 1 presents a comparative analysis of TAVR and SAVR along with primary outcomes from clinical trials of TAVR on low-risk patients.[21-23]
Aortic valve replacement surgical innovations
New surgical techniques and materials
In recent years, significant advancements and advancements have been observed in the domain of surgical procedures and materials employed in the context of SAVR. These advancements have resulted in improved patient outcomes and less invasiveness.
Minimally invasive techniques are gaining popularity, reducing the need for traditional sternotomies. These methods include mini sternotomy and small incisions in the chest or side, which, as previously stated, result in shorter hospital stays and quicker recoveries.[24] More durable and biocompatible prosthetic valves have been developed. Tissue-engineered valves and the use of bioprosthetic materials increased valve longevity and reduced the need for anticoagulation therapy.[25] While transcatheter techniques are a separate procedure, they have resulted in advancements in the field. TAVR-induced valve design innovation has resulted in valves that can be used in both TAVR and SAVR, expanding patient options.[2] Customized approaches that are tailored to patient-specific factors are also becoming more common. 3D printing technology enables surgeons to design custom prosthetic valves that fit and function better for individual patients.[26] The goal of specialized centers focusing solely on minimally invasive heart valve surgery is to provide patients with the most up-to-date surgical approaches and materials by combining expertise and technology.[27] In cases where patients need coronary artery bypass grafting (CABG), a combination treatment that includes SAVR is sometimes used at the same time. With this method, both procedures can be combined into one operation, which lessens the overall effect of surgery on the patient.[28]
Discoveries and improvements in the field have led to better outcomes for patients undergoing SAVR procedures. These improvements have made treatment choices and personalized care better.
Hybrid approaches: Justification and advantages
The integration of surgical and catheterization methods has yielded substantial advancements in the management of aortic valve disorders. The present study aims to investigate the integration of conventional open-heart surgery with minimally invasive catheter-based interventions.
The technique of TAVR or percutaneous aortic valve replacement has been extensively discussed in scientific literature. For instance, the StatPearls article on catheter management of aortic valve disorders provides a comprehensive overview of these procedures, elucidating their methodology, indications, contraindications, and potential complications.[29] TAVR is a minimally invasive procedure that offers an alternative to traditional open-heart surgery for the treatment of aortic valve disease. This innovative technique involves the insertion of a catheter through blood vessels, which is then guided to the heart to replace the damaged aortic valve with a new one. By avoiding the need for a large incision and direct access to the heart, TAVR presents a less invasive approach to aortic valve replacement.
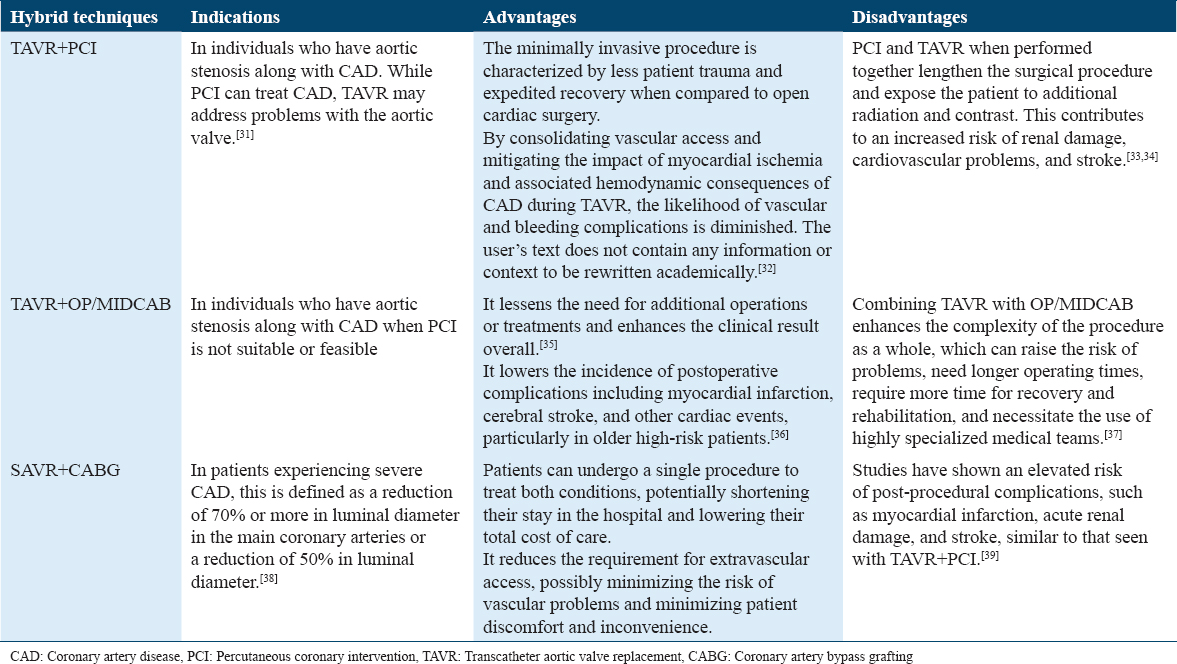
Hybrid techniques have been observed to be employed in various cardiovascular procedures, extending beyond valve replacement. This observation is emphasized in a scholarly article available on ScienceDirect, titled “Hybrid cardiovascular procedures.”[30] The article discusses the application of hybrid techniques in multiple cardiovascular interventions, such as CABG, percutaneous coronary intervention, and transcatheter valve therapy. Table 2 provides a comprehensive overview of various hybrid procedures, encompassing their respective indications, advantages, and disadvantages. Hybrid techniques have emerged as a promising avenue of exploration in various domains. Notably, hybrid epicardial/endomyocardial atrial fibrillation procedures and hybrid aortic arch debranching in conjunction with endovascular grafting for thoracic aortic procedures have garnered significant attention. These innovative approaches seek to combine the strengths of different methodologies to enhance treatment outcomes and improve patient care.
Comparison between different hybrid techniques in terms of morbidity and mortality is shown in Figure 2.
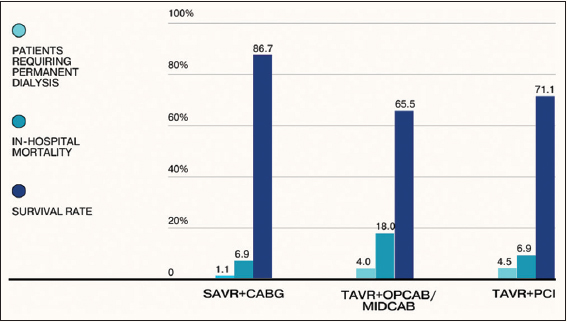
- Comparison between SAVR+CABG, TAVR+OP/MIDCAB, and TAVR+PCI. PCI: Percutaneous coronary intervention, TAVR: Transcatheter aortic valve replacement, CABG: Coronary artery bypass grafting
According to research findings, hybrid approaches provide patients with significant benefits. According to the 2012 ACCF/AATS/SCAI/STS Expert Consensus Document, this method has benefits for those with a variety of cardiovascular diseases.[40]
The TAVR program has been established by prestigious medical institutions, such as Tufts Medical Center, to offer hybrid procedures that combine the knowledge and expertise of cardiac surgeons and interventional cardiologists.[41] The integration of surgical and catheterization techniques has proved to be a revolutionary advance in the treatment of aortic valve disease. There are safer and more effective treatment options available, especially for high-risk patients, resulting in reduced invasiveness and enhanced patient outcomes.
Benefits in terms of patient outcomes and recovery
Hybrid approaches to aortic valve interventions, which combine surgical and catheter-based techniques, offer numerous benefits that enhance patient outcomes and recovery. These procedures are often less invasive than traditional open-heart surgeries, resulting in smaller incisions, reduced pain, and minimal blood loss.[42] Patients undergoing hybrid interventions typically experience faster recovery, leading to shorter hospital stays and a quicker return to daily activities. Moreover, the minimally invasive nature of these procedures reduces the risk of complications, making them a safer option for high-risk patients or those with multiple comorbidities. In certain cases, hybrid approaches preserve the sternum and chest wall, minimizing post-operative discomfort and complications related to sternal healing.[28] These interventions also allow for tailored treatments based on patient-specific factors and needs, providing an effective alternative for individuals with complex conditions, such as coronary artery disease (CAD), who may not be ideal candidates for traditional surgery.[35] Ultimately, the primary goal of hybrid techniques is to improve quality of life by relieving symptoms and minimizing risks, ensuring better outcomes for patients.[2]
Selection of patients and risk evaluation
Selection criteria for candidates for hybrid approaches
Hybrid approaches are advanced treatments performed on suitable candidates for the procedure to ensure the best possible results. The selection of candidates is based on clinical guidelines and expert consensus.
Individuals who exhibit significant narrowing of the aortic valves are very suitable candidates for hybrid procedures. The determination of whether intervention is necessary relies heavily on the degree of stenosis.[44] The consideration of hybrid procedures in patients who are deemed high-risk or ineligible for open cardiac surgery due to comorbidities, advanced age, or frailty necessitates a comprehensive assessment of the patient’s general health and risk factors to identify appropriate candidates.[35] Furthermore, it is imperative to take into account the patient’s preferences and values to ensure that the chosen intervention aligns with the patient’s expectations. Consequently, the process of shared decision-making among the patient, their family, and the medical team becomes crucial in determining the most suitable course of action.[2] The assessment of the aortic valve’s anatomical characteristics, such as its dimensions and configuration, is conducted to ascertain the feasibility of employing the hybrid technique.[44] Patients who have concomitant CAD may experience advantages from a hybrid strategy that integrates aortic valve intervention with coronary artery intervention. Various clinical standards, such as the guidelines established by the ACC/AHA, have been developed to assist in the identification of suitable candidates for therapy. Conforming to these guidelines helps facilitate the process of making informed decisions. The principles mentioned above establish the standards and suggestions for a range of interventions.[2] Hybrid techniques require the collaboration of a diverse team consisting of interventional cardiologists and cardiac surgeons to evaluate patient eligibility and ensure a thorough assessment.[9] High-risk patients undergo evaluation to determine the most effective intervention, and a thorough review of the risks and rewards is performed to strike a balance between prospective advantages and the hazards associated with these individuals. The assessment assists in determining the most suitable approach, whether it is surgical, transcatheter, or hybrid.[45-47]
Figure 3 illustrates the diverse criteria that contribute to the selection of the optimal treatment for specific patients.
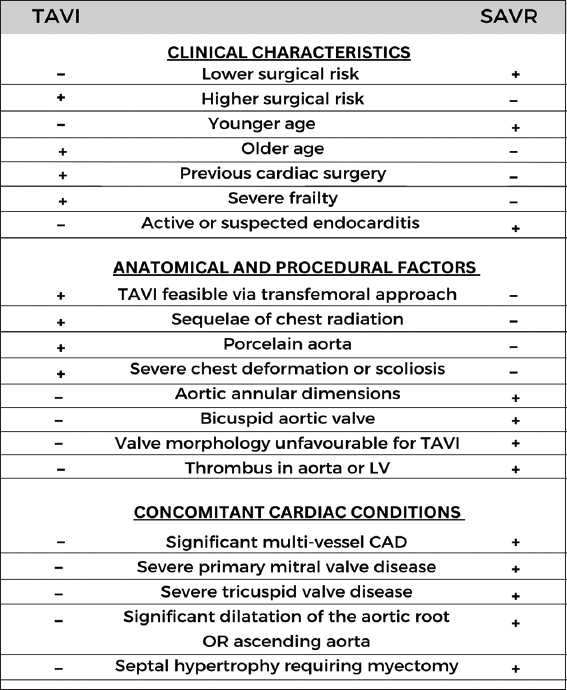
- Variables that have a role in treatment modality in an individual patient
Aortic valve hybrid procedure techniques
Aortic valve hybrid interventions offer a structured strategy designed for high-risk or complex cases by combining transcatheter and surgical procedures to replace or repair the aortic valve. A comprehensive patient examination is the first step in the procedure, which determines the patient’s general health, anesthetic suitability, and the degree of aortic valve disease. To identify the best course of action, multidisciplinary teams comprising cardiologists and surgeons examine each case. The architecture of the aortic valve, aortic root, and surrounding tissues are then assessed using advanced imaging techniques, such as computed tomography (CT) scans, to enable accurate operative planning.
The next step is to choose the best access location for the procedure’s transcatheter component. The apex of the heart or the femoral artery is a frequent access locations, depending on the anatomy of the patient and the type of valve prosthesis selected. To guarantee the optimum result, the type of valve – mechanical, biological, or transcatheter – is chosen based on anatomical considerations and patient-specific characteristics.
Using catheter-based procedures, the transcatheter valve is delivered to the aortic location through the selected access point throughout the procedure. Accurate deployment of the valve is guided by real-time imaging. Other surgical procedures like mitral valve repair or CABG can be required in specific circumstances. To manage concomitant heart diseases with minimal invasiveness, these surgical techniques are combined with the transcatheter method. For patients who need aortic valve intervention, this multimodal approach guarantees thorough and efficient therapy.
After valve deployment and any additional surgical steps, evaluate the valve’s function using imaging and hemodynamic assessment.
Close the access site(s) and monitor the patient during the recovery phase, ensuring hemodynamic stability and assessing for any complications.
This step-by-step approach to hybrid interventions combines the benefits of surgical precision with the minimally invasive aspects of transcatheter techniques, resulting in a customized solution for patients with aortic valve disease. To achieve the best results, a highly skilled and collaborative team of healthcare professionals is required.
Effectively integrating surgical and transcatheter components
Integrating surgical and transcatheter components effectively in hybrid techniques for aortic valve interventions is a difficult but critical approach that provides patients with tailored solutions. This integration combines surgical precision with the minimally invasive nature of transcatheter procedures, resulting in better patient outcomes.[35]
Long-term follow-up and clinical outcomes
Analyze patient outcomes following hybrid interventions
In various studies, patient outcomes following hybrid interventions for aortic valve disease have shown promising results. Several important findings and considerations are highlighted. Despite having a higher risk profile, patients with CAD who undergo TAVI have comparable outcomes to those without CAD.[48] Because of recent technological advances, both surgical and transcatheter therapies are now viable options. According to research, a multidisciplinary approach to decision-making is critical.[49] High-risk patients undergoing TAVR and SAVR have comparable long-term outcomes, specifically 5-year survival rates, according to an analysis of long-term outcomes. This demonstrates that TAVR is an effective alternative to SAVR.[50]
In the past, patients with symptoms of both diseases underwent simultaneous surgical procedures involving the replacement of the aortic valve (AVR) and the construction of coronary bypass grafts (CABG). However, it should be emphasized that hybrid solutions for the management of computer-aided design (CAD) are now available.[51] The efficacy and outcomes of TAVI versus SAVR in patients with severe aortic stenosis have been the subject of numerous systematic evaluations. Both evaluations have yielded substantial information regarding the efficacy of both techniques.[52] TAVI has the potential to increase post-procedural care and patient satisfaction by implementing patient care coordination programs along the TAVI pathway.[53]
Finally, hybrid interventions for aortic valve disease are evolving, providing tailored treatment options with promising outcomes. Multidisciplinary collaboration and patient-specific considerations are critical for successful post-procedural outcomes.
Monitoring and durability of hybrid techniques over time
Long-term monitoring and evaluation of hybrid techniques for aortic valve interventions are critical components of patient care and treatment success. These procedures, which combine surgical and transcatheter approaches, have evolved to effectively treat aortic valve conditions. Continuous monitoring and assessment are required to ensure long-term benefits and patient well-being.
The impact of structural valve degeneration (SVD) on the long-term durability of patients who undergo TAVI has been observed in empirical studies.[54] The bioprosthetic valves employed in these interventions have a propensity for SVD over time, necessitating periodic surveillance and evaluation.[55] Healthcare professionals utilize several imaging modalities and clinical evaluations to check the performance of valves and detect signs of deterioration. Furthermore, it is important to highlight that the ACC/AHA has placed considerable focus on assessing the long-term effectiveness of treatments and considering preventive approaches to avoid irreversible effects.[2,14] These recommendations provide a framework for assessing patient outcomes and monitoring the efficacy of hybrid techniques. To summarize, long-term monitoring and assessment of the durability of hybrid techniques for aortic valve interventions are critical to ensuring patients’ continued well-being and the long-term success of these procedures. This ongoing care and evaluation process requires regular follow-up, clinical assessments, and adherence to established guidelines.
Challenges and complications
For high-risk or complicated cases, hybrid aortic valve interventions – which mix transcatheter and surgical techniques – offer substantial advantages. Clinicians must carefully evaluate the difficulties and possible negative effects of these procedures, though. Among these, post-procedural issues like aortic regurgitation might impair the valve’s normal operation and necessitate further treatments. Prosthetic valve problems or vascular problems during the treatment can result in embolic consequences, including stroke, which is one of the most worrisome hazards. Vascular problems, such as bleeding and vascular damage at access sites, are very frequent issues that need careful attention and care. The results of aortic valve replacement may be worse for patients who also have CAD, which makes hybrid procedures much more difficult. In addition, because certain valve types are more likely to experience bleeding issues, bleeding associated with surgery and anticoagulation is a serious worry that is influenced by the type of valve implant used. Valve degeneration is another long-term issue that requires constant monitoring and may call for future re-interventions, especially with bioprosthetic valves. For patients with prosthetic valves, anticoagulation treatment is still crucial since it can be challenging to balance the risks of bleeding and thromboembolic events. Finally, a key factor in the success of hybrid aortic valve surgeries is patient selection. Finding the best candidates is a difficult and demanding procedure that calls for thorough consideration and judgment because these interventions are usually saved for high-risk instances.
Risk-mitigation and safety-improvement strategies
Various strategies, such as patient selection and risk assessment, have been developed to ensure safety and minimize complications. Risk assessment tools aid in the identification of candidates who will benefit the most from hybrid procedures. To ensure comprehensive evaluation, shared decision-making, and coordinated care, multidisciplinary teams are used.[2] The utilization of sophisticated imaging methodologies, such as three-dimensional echocardiography and computed tomography scans, enhances the process of preoperative preparation and intraoperative assistance, leading to a reduction in procedural mistakes. Minimally invasive surgical techniques, such as robot-assisted surgery, reduce trauma, shorten recovery times, and reduce the risk of complications.[43] Continuous training and simulation exercises are required for healthcare professionals involved in hybrid procedures to stay current with evolving technology and maintain their skills.[56-61] Ongoing research and innovation in device technology, such as transcatheter valve designs, contribute to improved hybrid intervention safety and efficacy. Postoperative monitoring is critical for detecting complications early. Regular follow-up ensures that patients receive prompt intervention when necessary, improving patient outcomes.[2] Healthcare providers can reduce complications, improve safety, and optimize outcomes for patients undergoing hybrid aortic valve interventions by implementing these strategies and emphasizing patient-centered care.
Imaging and Navigation Technology Integration
The role of advanced imaging techniques in hybrid procedure planning and execution
Advanced imaging techniques are critical in the planning and execution of hybrid procedures, particularly complex interventions such as aortic valve surgeries. These techniques provide accurate visualization and guidance throughout the procedure, increasing patient safety.
The importance of advanced imaging techniques begins with preoperative planning. Advanced imaging methods, such as 3D echocardiography, CT scans, and magnetic resonance imaging (MRI), provide detailed anatomical information about the patient’s heart and vasculature before the procedure. This assists surgeons in developing a comprehensive preoperative plan by assessing variables such as valve morphology, sizing, and positioning.[62] It also assists with intraoperative guidance. Real-time imaging during the procedure aids in device monitoring and placement. For catheter-based interventions, fluoroscopy, intravascular ultrasound, and transesophageal echocardiography (TEE) are used. All of this contribute to accurate valve deployment and reduce the risk of complications.[62] Advanced imaging techniques also aim to reduce radiation exposure for both patients and healthcare providers. Low-dose protocols and optimized imaging sequences help to maintain image quality while reducing radiation risks.[63] With high-quality images, surgeons can make real-time decisions, allowing them to adapt the procedure as needed and avoid unexpected complications. Finally, precise preoperative planning and intraoperative guidance may reduce complications, shorten procedure times, and improve patient recovery.
Making use of real-time navigation tools
The utilization of real-time navigation systems has been shown to improve patient outcomes and safety through the enhancement of surgical visualization and guidance. Real-time MRI represents a significant technological advancement. MRI enables direct observation of the aortic valve replacement procedure, a commonly employed technique in cardiac surgery that often involves a direct apical approach.[64] TEE is employed during TAVR to provide instantaneous imaging capabilities. The technology enables the positioning and supervision of devices.[65] The utilization of real-time MRI guidance during TAVR has been shown to enhance visibility, facilitate accurate deployment, and address the constraints associated with traditional imaging methods.[66] The implementation of real-time navigation tools has led to significant advancements in hybrid operations, resulting in enhanced safety and efficacy.
Collaboration of multidisciplinary teams
Aortic valve interventions have become increasingly complex, necessitating a multidisciplinary skill set to navigate the complexities involved. Surgeons bring surgical expertise, interventional cardiologists provide expertise in minimally invasive procedures, and imaging specialists provide real-time guidance through advanced imaging technologies such as MRI and TEE.
For the successful implementation of TAVI, collaboration between numerous stakeholders is of utmost importance. Collaboration between cardiac surgeons and interventional cardiologists is crucial for selecting the most appropriate technique and device for each patient. Simultaneously, imaging specialists play a vital role by providing immediate feedback to facilitate precise device placement.[67]
Case studies and decision-making procedures
Case conferences enable multidisciplinary teams of surgeons, interventional cardiologists, and other specialists to assess the patient’s unique condition. They provide a forum for experts to share knowledge, assess risks, and tailor treatment plans to individual needs. This collaborative approach ensures that all points of view are taken into account, resulting in more informed decisions.[68]
Furthermore, these discussions allow the best hybrid technique for aortic valve interventions to be chosen. For example, in TAVR, the decision to perform this minimally invasive procedure, which is often reserved for high-risk or inoperable patients, is critical and benefits from a collective risk-benefit assessment.[69]
Effective decision-making processes, which are frequently supported by guidelines and criteria, aid in aligning the medical team’s efforts with the best interests of the patient. They also ensure that patients are active participants in their healthcare journey, which is increasingly important.
Finally, the value of case discussions and decision-making processes in hybrid aortic valve interventions cannot be overstated. They promote collaboration, improve individualized patient care, and contribute to improved outcomes in a field where precision and expertise are critical.
Cost-effectiveness and economic considerations
Assessing the economic impact of hybrid techniques
In modern healthcare, the economic impact of hybrid techniques for aortic valve interventions is critical to consider. TAVI and hybrid surgical procedures, for example, aim to improve patient outcomes while also addressing economic concerns. TAVI’s clinical effectiveness and cost-effectiveness are compared to traditional surgical approaches in certain studies, such as a health technology assessment. These evaluations help determine whether TAVI is cost-effective in treating aortic stenosis.[70] The studies aim to determine the financial impact of implementing TAVI in healthcare systems. This includes determining the costs of implementing these techniques as well as their long-term effects on healthcare budgets.[71] Patient outcomes are taken into account alongside economic factors. The benefits of improved patient health and quality of life are balanced against the costs of implementing the techniques.[72]
A cost-effectiveness comparison with traditional approaches
Cost-effectiveness analysis (CEA) is critical in assessing the economic implications of using hybrid techniques versus traditional approaches in a variety of fields, including healthcare.
CEA evaluates whether innovative hybrid interventions, such as hybrid surgical procedures or advanced medical therapies, provide better value for money than conventional treatments in healthcare. For example, studies on the cost-effectiveness of hybrid closed-loop therapy for type 1 diabetes patients have shown that it has the potential to be more cost-effective than traditional treatment regimens.[73] CEA entails weighing the relative costs and outcomes of various courses of action. It assists decision-makers in making informed decisions by taking into account not only clinical effectiveness but also the economic impact of new technologies or techniques. The World Health Organization provides guidelines for conducting CEA to ensure rigorous and standardized cost-effectiveness assessments of healthcare interventions.[74]
Future research and directions
The most recent trends and advancements in hybrid techniques can be summarized as a shift toward patient-centered care with a focus on personalized treatment strategies. The appropriate treatment is determined by a multidisciplinary team that assesses the particular characteristics of the patient. In recent years, there have been significant advancements in the field of minimally invasive procedures. TAVR and valve-in-valve TAVR have emerged as the preferred therapeutic interventions for patients who face an increased risk during surgical procedures.[75] Moreover, previous studies have provided evidence to support the notion that the utilization of hybrid procedures might effectively expand the range of therapy options available for patients who are deemed high-risk or inoperable. The broadening of intervention capabilities has led to the emergence of innovative approaches, such as valve-in-valve TAVR, which offer different therapeutic possibilities for individuals who were previously deemed untreatable.[76]
The development of hybrid operating rooms (ORs) with advanced imaging capabilities has improved procedure precision.[77] For patients with complex aortic pathologies, hybrid total thoracic aortic repair, which combines endovascular stent grafting with surgical approaches, is emerging as a viable option. This technique provides a less invasive option for treating aortic disease.[76] Ongoing research looks into how bioengineered tissues and materials can be integrated into hybrid procedures. These advancements may pave the way for the development of more durable and long-lasting valve replacements, reducing the need for repeat interventions. These developments are reshaping the landscape of aortic valve disease management, providing more options and better outcomes for patients with a wide range of clinical profiles.
Conclusion
The development of hybrid techniques for aortic valve interventions appears to be a promising field in cardiology. To address current challenges and improve patient outcomes, more research and innovation in this area are needed.
The development of hybrid techniques for aortic valve interventions appears to be a promising field in cardiology. To address current challenges and improve patient outcomes, more research and innovation in this area are needed. Continuous research into the design and improvement of transcatheter heart valves is essential. Material, durability, and delivery system advancements can lead to more effective and safer procedures, expanding the patient population that can benefit from hybrid techniques. Better predictive models and criteria can assist in identifying which patients are most likely to benefit from hybrid interventions, avoiding unnecessary procedures and improving outcomes. A critical area of research is the advancement of minimally invasive approaches. Shorter hospital stays, faster recovery, and lower complication rates can all be achieved by reducing the invasiveness of hybrid procedures. New access routes and techniques should be investigated. Improving imaging and navigation tools in hybrid ORs can improve procedural precision. The goal of bioengineered tissue and valve solutions research is to create more durable and long-lasting valves. Long-term outcomes of hybrid procedures require more research. Long-term evaluation of the durability and functional status of valves, as well as the incidence of valve-related complications, is critical for determining the success of these interventions. It is critical to create hybrid training programs for healthcare professionals. As the field evolves, it is critical to ensure that clinicians have the necessary skills and knowledge to provide safe and effective care. The impact of hybrid interventions on patients’ daily lives and overall well-being should be prioritized in research. It is necessary to pay close attention when navigating regulatory approvals and reimbursement policies for hybrid procedures. Collaboration with regulatory bodies and insurance providers is critical to ensuring patient access to these cutting-edge treatments.
Author’s Declaration Statements
Author contributions
Fnu Fariha, Muhammad Ali Muzammil, Muhammad Usama Shahid, Muhammad Haseeb: Conceptualization, methodology, software, data curation, validation, writing - original draft preparation. Merceline Eugène, Mohammed Rafea Adnan Shukri, Daniyal Abbasi: Writing - Reviewing and editing, project administration. Majid Suleman: Writing - reviewing and editing, supervision.
Acknowledgments
Open Access funding is provided by the Qatar National Library.
Conflicts of Interest/Disclosures
The authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest. The authors declare that they have no conflicts of interest.
Funding
The authors report no external funding.
References
- 2020 ACC/AHA guideline for the management of patients with valvular heart disease:A report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2021;143:e72-227.
- [Google Scholar]
- Aortic Regurgitation. 2023. StatPearls-NCBI Bookshelf. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555944
- [Google Scholar]
- Anatomy of the aortic valvar complex and its implications for transcatheter implantation of the aortic valve. Circ Cardio Inter. 2008;1:74-81.
- [Google Scholar]
- Aortic Stenosis:Practice Essentials, Background, Pathophysiology. Available from: https://emedicine.medscape.com/article/150638-overview
- [Google Scholar]
- Aortic Valve Replacement. 2023. StatPearls-NCBI Bookshelf. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537136
- [Google Scholar]
- Anatomy, Thorax, Aortic Valve. 2022. StatPearls-NCBI Bookshelf. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559384
- [Google Scholar]
- The development of transcatheter aortic valve replacement (TAVR) Global Cardiol Sci Pract. 2016;4:e201632.
- [Google Scholar]
- Aortic valve and ascending aorta guidelines for management and quality measures:Executive summary. Ann Thorac Surg. 2013;95:1491-505.
- [Google Scholar]
- Evolving indications of transcatheter aortic valve replacement compared to surgical valve replacement:A review of the current literature. Cureus. 2022;14:e23364.
- [Google Scholar]
- Stanford Health Care;(n.d.) Available from: https://stanfordhealthcare.org/medical-treatments/t/transcatheter-aortic-valve-replacement-tavr.html
- [Google Scholar]
- Nationally representative repeat transcatheter aortic valve replacement outcomes:Report From the centers for medicare and medicaid services. JACC Cardiovasc Interv. 2021;14:1717-26.
- [Google Scholar]
- Comparing traditional aortic valve surgery and transapical approach to transcatheter aortic valve implant. Eur Heart J. 2020;22(Suppl E):E7-12.
- [Google Scholar]
- Comparison of outcomes after transcatheter aortic valve replacement vs surgical aortic valve replacement among patients with aortic stenosis at low operative risk. JAMA Netw Open. 2019;2:e195742.
- [Google Scholar]
- Outcomes comparison of different surgical strategies for the management of severe aortic valve stenosis:Study protocol of a prospective multicentre European registry (E-AVR registry) BMJ Open. 2018;8:e018036.
- [Google Scholar]
- Transcatheter versus surgical aortic valve replacement in severe, symptomatic aortic stenosis. J Geriatr Cardiol JGC. 2018;15:76-85.
- [Google Scholar]
- Cost-effectiveness of transcatheter versus surgical aortic valve replacement in patients with severe aortic stenosis at intermediate risk. Circulation. 2019;139:877-88.
- [Google Scholar]
- A comparative profitability analysis of transcatheter versus surgical aortic valve replacement in a high-volume French hospital. Health Econ Rev. 2019;9:6.
- [Google Scholar]
- CTG Labs-NCBI;(n.d.-b). Available from: https://clinicaltrials.gov/study/NCT02675114
- CTG Labs-NCBI;(n.d.-c). Available from: https://clinicaltrials.gov/study/NCT02701283
- CTG Labs-NCBI;(n.d.-d). Available from: https://clinicaltrials.gov/study/NCT01057173
- Recent advances in aortic valve replacement. F1000Res. 2019;8:F1000. Faculty Rev-1159
- [Google Scholar]
- Antithrombotic treatment after surgical and transcatheter heart valve repair and replacement. Front Cardiovasc Med. 2021;8:702780.
- [Google Scholar]
- Technology for new surgical aortic valve replacement:Current evidence and future directions. J Thorac Dis. 2018;10:6392-5.
- [Google Scholar]
- Updates on the latest surgical approach of the aortic stenosis. J Clin Med. 2021;10:5140.
- [Google Scholar]
- Surgical approaches to aortic valve replacement and repair-insights and challenges. Interv Cardiol. 2014;9:32-6.
- [Google Scholar]
- Catheter Management of Aortic Valve Disorders. 2023. StatPearls-NCBI Bookshelf. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538169
- [Google Scholar]
- Percutaneous coronary intervention in transcatheter aortic valve implantation patients:Overview and practical management. Front Cardiovasc Med. 2021;8:653768.
- [Google Scholar]
- Severe aortic stenosis and coronary artery disease--implications for management in the transcatheter aortic valve replacement era:A comprehensive review. J Am Coll Cardiol. 2013;62:1-10.
- [Google Scholar]
- Impact of coronary artery disease and percutaneous coronary intervention on outcomes in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation. EuroIntervention. 2011;7:541-8.
- [Google Scholar]
- First experience with transcatheter aortic valve implantation and concomitant percutaneous coronary intervention. Clin Res Cardiol. 2011;100:311-6.
- [Google Scholar]
- Transcatheter aortic valve replacement- management of patients with significant coronary artery disease undergoing aortic valve interventions:Surgical compared to catheter-based approaches in hybrid procedures. BMC Cardiovasc Disord. 2019;19:108.
- [Google Scholar]
- Concomitant anaortic OPCAB and transfemoral TAVR for high-risk patients:A case series. J Cardiac Surg. 2022;37:3935-42.
- [Google Scholar]
- Hybrid minimally invasive approach for combined obstructive coronary artery disease and severe aortic stenosis. Innovations (Phila). 2020;15:131-7.
- [Google Scholar]
- UpToDate;(n.d.-c). Available from: https://www.uptodate.com/contents/indications-for-valve-replacement-for-high-gradient-aortic-stenosis-in-adults
- Aortic valve replacement after bypass surgery:Surgical (SAVR) or transcatheter (TAVR) J Thorac Dis. 2017;9:2714-5.
- [Google Scholar]
- 2012 ACCF/AATS/SCAI/STS expert consensus document on transcatheter aortic valve replacement. J Am Coll Cardiol. 2012;59:1200-54.
- [Google Scholar]
- MA-Tufts Medical Center;(n.d.). Available from: https://www.tuftsmedicalcenter.org/patient-care-services/departments-and-services/cardiovascular-center/clinical-care-services/tavr
- Hybrid intervention approach to coronary artery and valvular heart disease. Proc (Bayl Univ Med Cent. 2020;33:520-3.
- [Google Scholar]
- Patient selection for transcatheter aortic valve replacement:A combined clinical and multimodality imaging approach. World J Cardiol. 2017;9:212-29.
- [Google Scholar]
- Transcatheter aortic valve implantation and off-pump coronary artery bypass surgery:An effective hybrid procedure in selected patients. Interact Cardiovasc Thorac Surg. 2018;27:102-7.
- [Google Scholar]
- Transcatheter Aortic Valve Implantation for Severe Aortic Stenosis-Overcoming the Challenges. 2020. Radcliffe Cardiology. Available from: https://www.icrjournal.com/articles/transcatheter-aortic-valve-implantation-severe-aortic-stenosis-overcoming-challenges
- [Google Scholar]
- Impact of coronary artery disease on outcomes of severe aortic stenosis treatment with transcatheter aortic valve implantation. Postepy Kardiol Interwencyjnej. 2019;15:167-75.
- [Google Scholar]
- Percutaneous versus surgical intervention for severe aortic valve stenosis:A systematic review. Biomed Res Int. 2021;2021:3973924.
- [Google Scholar]
- Transcatheter aortic valve replacement programs:Clinical outcomes and developments. J Am Heart Assoc. 2020;9:e015921.
- [Google Scholar]
- Management of coronary artery disease in patients with aortic stenosis in the era of transcatheter aortic valve replacement. Front Cardiovasc Med. 2023;10:1139360.
- [Google Scholar]
- Transcatheter aortic valve implantation against conventional aortic valve replacement surgery in high-risk patients with aortic stenosis;a cost-effectiveness analysis. Health Econ Rev. 2023;13:1.
- [Google Scholar]
- The COORDINATE pilot study:Impact of a transcatheter aortic valve coordinator program on hospital and patient outcomes. J Clin Med. 2022;11:1205.
- [Google Scholar]
- Long-term valve durability in patients undergoing transcatheter aortic valve implantation. Heart Lung Circ. 2023;32:240-6.
- [Google Scholar]
- Midterm Durability and structural valve degeneration of transcatheter aortic valve replacement in a federal facility. Innovations (Phila). 2022;17:382-91.
- [Google Scholar]
- High risk aortic valve replacement-the challenges of multiple treatment strategies with an evolving technology. Ulster Med J. 2016;85:18-22.
- [Google Scholar]
- Prosthetic heart valves:Selection of the optimal prosthesis and long-term management. Circulation. 2009;119:1034-48.
- [Google Scholar]
- Complications after aortic valve repair and valve-sparing procedures. Ann Cardiothorac Surg. 2013;2:130-9.
- [Google Scholar]
- Transcatheter aortic valve replacement in the catheterization laboratory versus hybrid operating room:Insights from the FRANCE TAVI registry. JACC Cardiovasc Interv. 2018;11:2195-203.
- [Google Scholar]
- Prosthetic aortic valves:Challenges and solutions. Front Cardiovasc Med. 2018;5:46.
- [Google Scholar]
- 2022. Aortic Valve Repair and Aortic Valve Replacement-Mayo Clinic. Available from: https://www.mayoclinic.org/tests-procedures/aortic-valve-repair-aortic-valve-replacement/about/pac-20385093
- Advanced imaging in interventional cardiology:Mixed reality to optimize preprocedural planning and intraprocedural monitoring. Kardiol Pol. 2021;79:331-5.
- [Google Scholar]
- The impact of dependence on advanced imaging techniques on the current radiology practice. Ann Med Surg (Lond). 2022;78:103708.
- [Google Scholar]
- Real-time interactive MRI-guided cardiac surgery:Aortic valve replacement using a direct apical approach. Magn Reson Med. 2006;56:958-64.
- [Google Scholar]
- Imaging in Transcatheter aortic valve replacement (TAVR):Role of the radiologist. Insights Into Imaging. 2014;5:123-45.
- [Google Scholar]
- Real-time magnetic resonance imaging-guided transcatheter aortic valve replacement. J Thorac Cardiovasc Surg. 2016;151:1269-77.
- [Google Scholar]
- Collaboration between Interventional Cardiologists and Cardiac Surgeons in the Era of Heart Team Approach. London: InTech eBooks; 2017.
- [Google Scholar]
- Hybrid Cardiovascular Therapy:Interventional (and Surgical) Procedures in High-risk Patients;(n.d.) Available from: https://www.openaccessjournals.com/articles/hybrid-cardiovascular-therapy-interventional-and-surgical-procedures-in-highrisk-patients.html
- [Google Scholar]
- TAVI Intervention:Risks, Case Studies, Procedure-Mauro Cassese. 2021. Mauro Cassese-Specialista in Chirurgia Generale E Cardiochirurgia. Available from: https://www.maurocassese.com/tavi-intervention-risks-case-studies-procedure
- [Google Scholar]
- Ontario Health (Quality). Transcatheter aortic valve implantation in patients with severe, symptomatic aortic valve stenosis at intermediate surgical risk:A health technology assessment. Ont Health Technol Assess Ser. 2020;20:1-121.
- [Google Scholar]
- Transcatheter aortic valve implantation versus surgical aortic valve replacement for severe aortic stenosis:Results from an intermediate risk propensity-matched population of the Italian OBSERVANT study. Int J Cardiol. 2013;167:1945-52.
- [Google Scholar]
- Transcatheter aortic valve implantation for the treatment of severe symptomatic aortic stenosis in patients at very high or prohibitive surgical risk:Acute and late outcomes of the multicenter Canadian experience. J Am Coll Cardiol. 2010;55:1080-90.
- [Google Scholar]
- Cost-effectiveness analysis of a hybrid closed-loop system versus multiple daily injections and capillary glucose testing for adults with type 1 diabetes. Diabetes Technol Ther. 2020;22:812-21.
- [Google Scholar]
- 2003. Making Choices in Health:WHO Guide to Cost-Effectiveness Analysis. Available from: https://apps.who.int/iris/handle/10665/42699
- Transcatheter aortic valve implantation in the United Kingdom. Circulation. 2015;131:1181-90.
- [Google Scholar]
- Hybrid thoracic aortic repair and aortic valve-in-valve replacement for chronic type a dissection. Thorac Cardiovasc surgeon Rep. 2023;12:e17-e20.
- [Google Scholar]
- 2015. American College of Cardiology. Available from: https://www.acc.org/latest-in-cardiology/articles/2015/04/27/11/05/clinical-advances-with-hybrid-surgical-technologies




