
Translate this page into:
Comparison of chondrosarcoma cases: current clinical situations among institutions
Address for correspondence: Shi Jiandang, Department of Spinal Surgery, General Hospital of Ningxia Medical University, Ningxia Medical University 804 Shengli Street, Xingqing District, Yinchuan, 750004, Ningxia, People’s Republic of China. E-mail: shi_jiandang@163.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Qassim Uninversity and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective:
Chondrosarcoma is a rare tumor that has a variable biological characteristic, and its treatment is controversial. We performed a comparison review of different regional institutions series to assess the clinical outcome of patients.
Methods:
A retrospective review of 33 chondrosarcomas (Grades I, II, and III) patient data since 2013, compared with 15 author’s total 868 patients published literature results to find more about clinical and statistical advantages and similarities with author institute cases. Here is the mentioning of clinical information, surgery type categorized, adjuvants types, genders, follow-up years, recurrence, affected areas, death rates, successful outcome, and survival rates using statistical methods.
Results:
The overall survival rate was 94%, successful outcome 85% in 4.3±1.2 years follow-up. Observed wide resection, distilled water as adjuvant, chemo and radiotherapy significantly shows excellent results over our compared chondrosarcoma literature data. We have also marked that females and humerus bone are more affected by chondrosarcoma among those literature data.
Conclusions:
Low-grade chondrosarcoma of the skeleton can be treated with wide resection. Using distilled water give good oncological outcome and a very low rate of post-surgical complications for chondrosarcoma all grades recurrence.
Keywords
Chondrosarcoma
clinical
comparison
extremity cases

Introduction
Chondrosarcoma is the second most common malignant tumor of the skeleton. Chondrosarcoma is a rare cancer with an estimated incidence of 1 in 200,000 per year.[1] The tumors have considerable variation in outcome depending on size, histologic grade, Musculoskeletal Tumor Society stage,[2] and tumor type. All kinds of tumors have different characteristics and biological differences. Chondrosarcoma grade and the anatomical site are important because both influence the sort of treatment and result. The chondrosarcoma can affect any part of the bone but has a predilection for the pelvis, femur, and proximal humerus.[3] Surgery procedures do not always recommend treatment; neither chemotherapy nor radiation therapy is effective in this tumor.[4] For this tumor male prevalence of two: One, and this usually occurs in the third and fifth decades of a lifetime.[5,6] This tumor of the pelvis is the most aggressive and has the lowest survival rate.[7,8] Chondrosarcomas are malignant cartilaginous neoplasms with distinct morphological features and clinical behavior. Among all primary malignant tumors of the skeleton, this rare tumor is 20%.[9] People still making wrong decisions because of a lack of awareness about the treatment of their tumors. So that the survival rate is low and the health-care system could not help big numbers of people who do not come to hospitals for treatment, but they waste time with quacks or bonesetters. It happens because of many social and cultural factors that patient continues to visit such peoples.[10] The motive of this research is to the comparison among regions of chondrosarcoma patient’s cases. The goal of this article is not to discuss our accuracy or outcome of chondrosarcoma grades, notwithstanding to look for the weight of the information come up with their clinical information and history, surgical, survival rate, infections, complications, functional, and gender for better analytical clinical understanding.
Surgical and treatment information
Surgical treatments are mainly recommended for most types of chondrosarcoma, and probably surgery used for a newly diagnosed tumor or if recurrence occurs. Particular treatment for chondrosarcoma will be a definite healthcare provider based on overall health, medical history, Type, stage (extent), cancer location, age, tolerance for specific medicines, procedures, different therapies, course of the disease and its expected result, patient’s opinions, and preferences. Enormous of authors suggested wide resections for grade two and three tumors for extra compartmental Grade 1 lesion.[4,11,12] Few authors recommend wide resection, while others are convinced by intralesional resection augmented with a surgical adjuvant, such as LN2, C6H5OH (phenol), electrocautery, and argon-beam laser, is adequate.[13,14] Unfortunately, biopsy in the chondral intramedullary lesion is not reliable.[15,16] Tumor grading often misleads the surgeon to inapplicable surgery. Clinical history and imaging studies are significant when choosing the appropriate surgical technic. We have done 17 wide angel resection, seven marginal resections, and two intralesional resections. We collected the age, gender, follow-up (months), anatomical locations, staging according to the Enneking system.[17] Follow as a usual pre-operative surgical procedure in our hospital according to the patient’s present situation and body conditions. During surgeries, the patient’s position for the spine was the prone and supine position for extremity. The target for the treatment is to remove the mass and reduces the possibility that it will cause recurrence. The following kinds of surgeries may be used:
Resection, Curettage, Bone cement, Limb-sparing surgery, Amputation, Reconstructive surgery, and Biopsy. Several authors agree to use this technique for tumor cells.[18] The tumor cells will be inactive in due course sop in distilled water for 60 s at 55°C, and the tumor cell death rate was 100%. Tumor cells can be destroyed by distilled water for 60 s at 55°C, which is proved in several author’s literature. This way of treatment provides a new fast and low-cost tumor-free technic to inactivate tumor cells, as well as attached to surgical instruments.[18] However, in some cases of chondrosarcoma tumor, intralesional excision may not be adequate, for example, because of an intra-articular or pelvic localization or large size.[19] In some cases, a greater tendency to metastasize or progress occurs with axial-pelvic tumors, which also have higher local recurrence rates.[20] There are 14 fracture cases; we believe that the fractures occur more because of a lack of osteosynthesis, although there is no enough data to prove it. The distinction between wide resection and marginal resection was based on a combination of the pathology report and the operative note. Each of these techniques carries different risks and benefits. Furthermore, with the development of medical science, everyday new methods and techniques are used by doctors, which outcome is slightly better and efficient. In our hospital, we have followed all pre-surgical procedures according to Chinese medical ethics, rules, and regulations. See the surgical procedures chart in Figure 1.
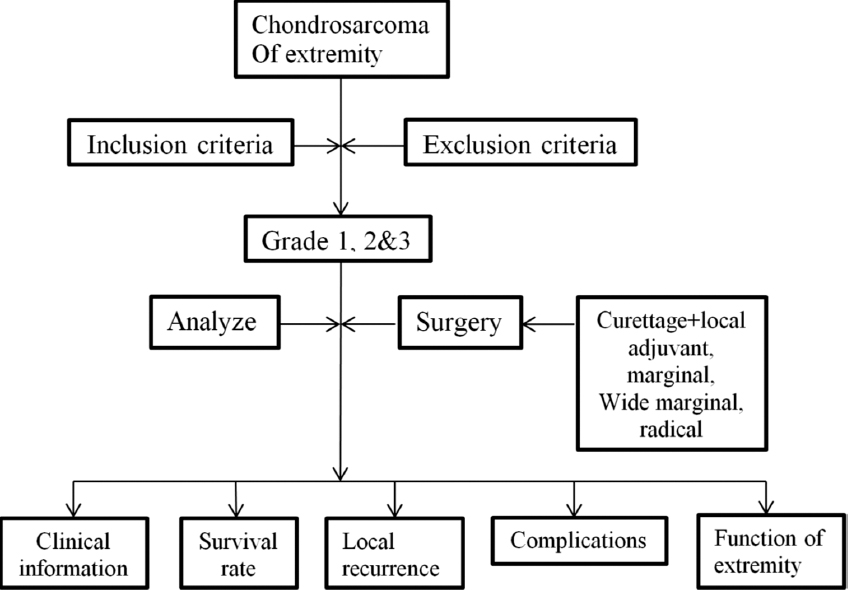
- Flowchart of chondrosarcoma surgical management
Post-operative follow-up
Patients come for evaluation in the first 2 years every 3 months once, the next 5 years every 6 months once, and annually once after that. Radiographs and physical exam were performed at each time. If local recurrence was suspected, then additional imaging was requested, such as a computed tomography (CT) scan or magnetic resonance imaging. Chemotherapy and radiotherapy were used for a few malignant tumor patients. If there is lung metastasis, then determine with CT. Tumor margins were evaluated accordingly. Cost of the potential immediate post-surgical neurologic deficits against the advantage of long-term survival should factor heavily into the treatment strategy, also taken part in decision making with the patients.
Radio and chemotherapy
If chondrosarcoma tumors cannot be removed with surgical procedures, then external beam radiotherapy may be used to treat it. This therapy may apply to destroy any cancer cells after wide resection, which is left behind. Radiotherapy is also used if the tumor is a recurrence. Based on the skull or in the spinal bones tumor treat by apply of conformal proton beam radiation therapy or intensity-modulated radiation therapy. For low-grade chondrosarcoma, usually chemotherapy not use due to showing no improved survival rate.
Another minimal invasive percutaneous technique is radiofrequency ablation, which is used mainly for palliating painful bone metastasis.[21,22] However, we have not done any study or addressing the application of this technique in tumors and, more specifically, chondrosarcoma tumors.
Methods and Design
We conducted a formal review of any published literature from the past 23 years related to chondrosarcoma types and grades in internet-based journals were performed to optimize capture all relevant studies. The strength of evidence was then graded for each chondrosarcoma measure. The level of evidence for our studies collects from 15 author’s institution research papers with a total of 868 patients for comparison with our patient’s data. The tumor grading was collected from the files of the hospital database, which was completed. Patients treated in the author’s institution for all grade chondrosarcoma of bones from 2012 to 2018 were performed as a retrospective review. This study was approved by the Hospital and University ethical committee for clinical research; also informed consent was gathered from the patients participating.
Literature selection criteria
Inclusion criteria
(1) Cases of chondrosarcoma, different grades chondrosarcoma, the oncologic outcome of chondrosarcoma tumors using adjuvants; (2) the literature was divided into experimental group and control group based on chondrosarcoma grades; and (3) prospective cohort study, systemic analysis, case-control studies or series, expert opinions. The inclusion data were based on the extracted directory from the full database records.
Exclusion criteria
(1) Few patients were kept out from the current study because the follow-up was <24 months or lack of clinical data; (2) if the literature data are incomplete and cannot be extracted; (3) if repeated publications; and (4) if the article format is a review, case report, or not meet the inclusion criteria.
Literature selection
The system searches major foreign databases, such as PubMed, CNKI, Baidu, Ovid, Google Scholar, Cochrane Library, Research Gate, and EMBASE from 2018-05-30. The keywords were for search: Chondrosarcoma, chondrosarcoma types, chondrosarcoma grade, chondrosarcoma cases, chondrosarcoma meta-analysis, and the surgical technique of chondrosarcoma.
Manually select major orthopedic journals and recent review references; ask colleagues to understand the results of the completed but unpublished literature and related experimental results of the unfinished experiment to expand the search of the references included in the original literature. Literature screening was performed independently by two authors. If the screening results are inconsistent, the third author decides the screening results and contacted.
All data are cross-checked.
Results
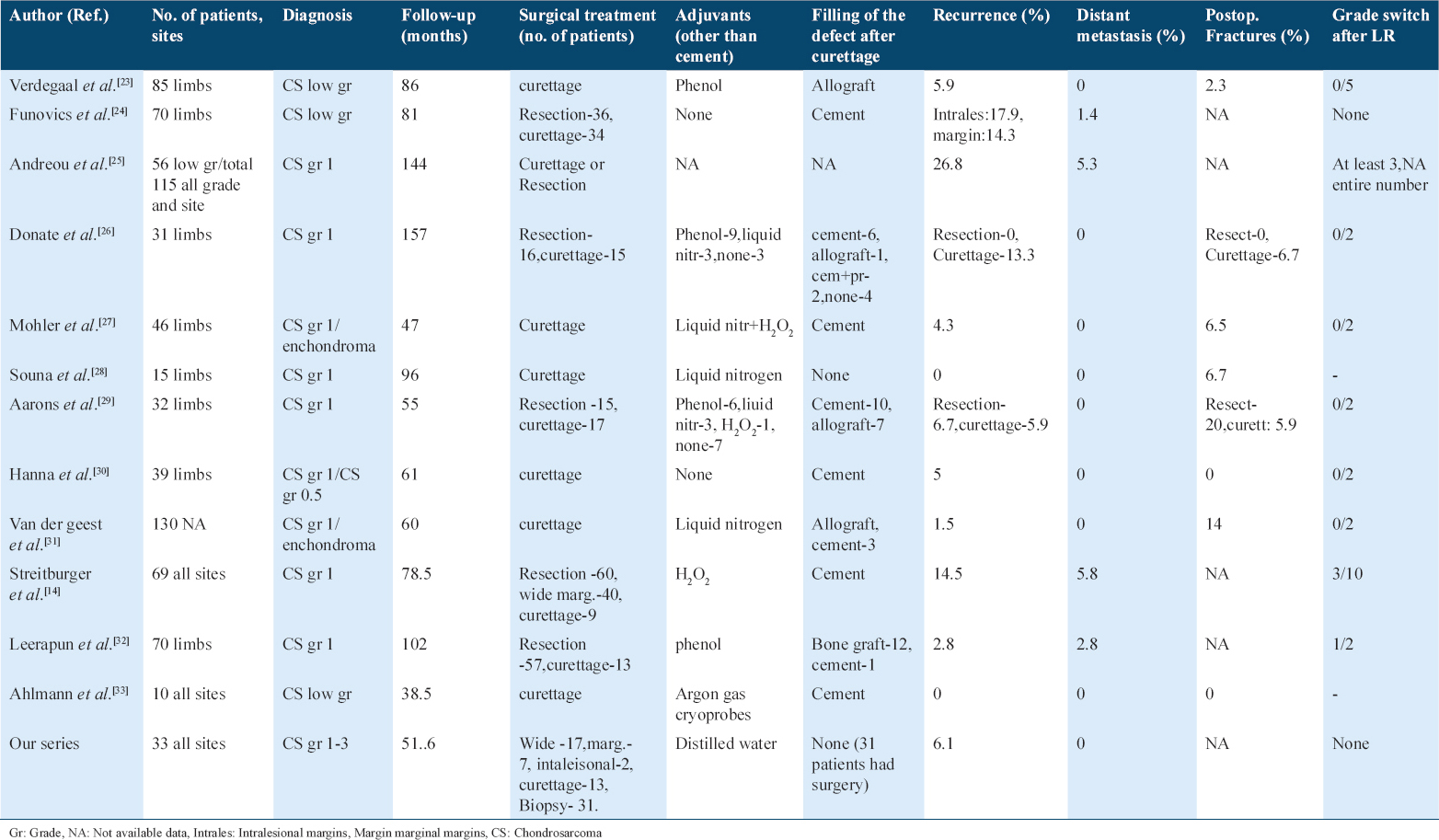
We have found that using distilled water as an adjuvant during tumor surgeries has an excellent effect. The authors used distilled water for all kinds of chondrosarcoma surgeries. Only 6.1% of our patient’s tumor recurrence but did not switch their chondrosarcoma grades from one to another. Distilled water shows better outcomes (survived 31 patients) over phenol, liquid nitrogen, or H2O2 as an adjuvant in all of our patient’s surgeries, which is one of the most significant founding in our study than other authors. Hence, the authors suggested using distilled water combined with all major surgical techniques; especially wide resection may have better outcomes.
There are 17 wide resections in this study [Tables 1 and 2] and mentioned that author has used distilled water for all of the surgeries. Besides, the overall results of survival and success rate are greatly influenced by it. Hence, it could be an important point/data to prove that distilled water has a significant connection with this study outcome.
Furthermore, we have seen that wide resection may help chondrosarcoma patients achieve a high survival rate in 5–10 years follow-up with 85% successful outcome.
In other regions, according to the author’s literature [Tables 1 and 3], we have found that female patients are affected more by chondrosarcoma than our area, which is different from the previous chondrosarcoma literature studies.
There are 17 wide resections in this study [Tables 1 and 2] and mentioned that author has used distilled water for all of the surgeries. Besides, the overall results of survival and success rate are greatly influenced by it. Hence, it could be an important point/data to prove that pre- and post-operative surgery, our patients take chemotherapy and radiotherapy, which is slightly different from other region’s treatments; it may help achieve a highly successful outcome with avoiding the minimum death rate. Although, the author did not include much information about this due to this study focus on overall chondrosarcoma surgical and survival outcomes only.
Statistical data comparison total 901 patients [Tables 1 and 3] show that most patients affected by chondrosarcoma on limb area of their body among all of the literature.
There is 0% distant metastasis among our patients.
There are no deep infections occurred besides the case mentioned above after surgery.
After intercalary resection of the humerus was seen stress fracture of the vascularized fibular graft and heal spontaneously with conservative treatment in one case.
The incidence of complications was significantly higher in the resection group (Fisher’s exact test: 0.0007). However, doctors treat all of the patients without any serious incidence under close monitoring of burn units.
Statistical Information and Analysis
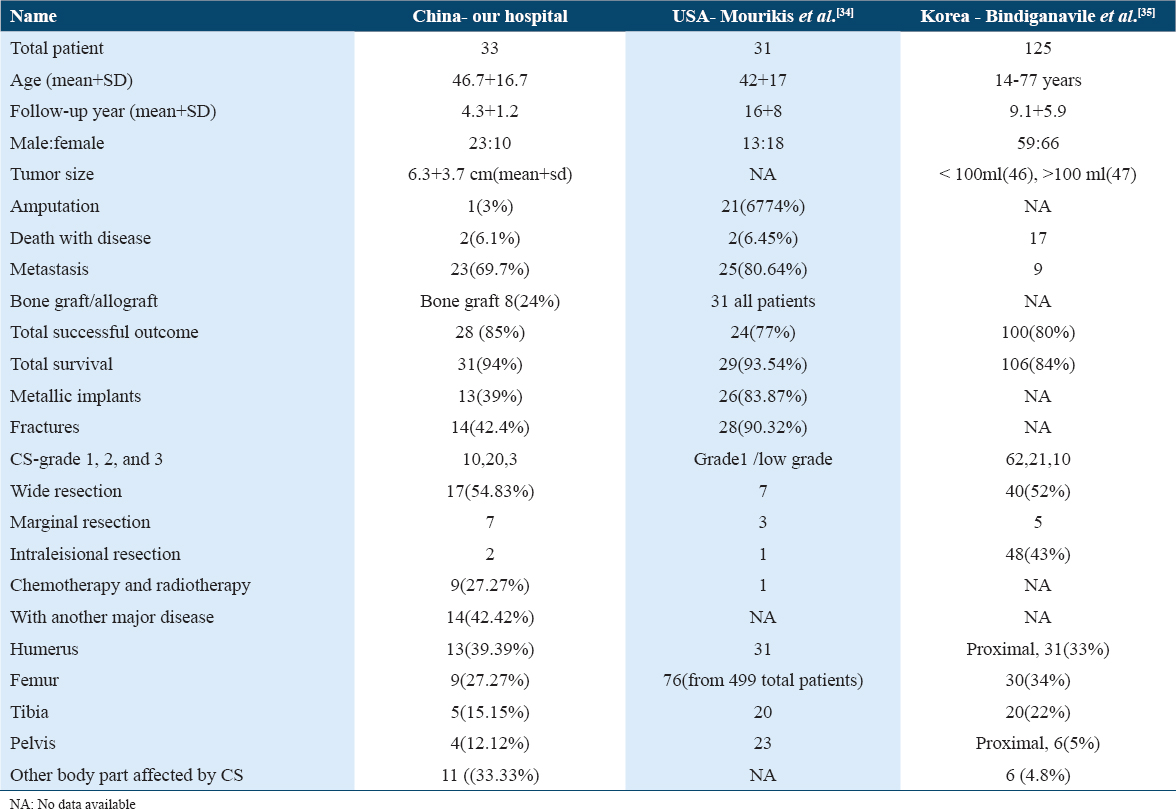
SPSS v24.0 was used to perform the statistical analyses for the patient’s data. In this study, author has compared all grades of chondrosarcoma patient’s data with 13 author’s chondrosarcoma published research literature from different regions in Table 1, and two authors in Table 2. A total of 15 author’s research literature and a total of 868 patients were included for comparison. Time and age intervals were regarded as continuous variables.
Analysis results
Tables 1 and 3 recorded a total of 15 authors and their literature included factors are below: author’s name, gender, type of tumor, locations and diagnosis of tumor, years (months) follow-up, age, surgical procedures, types of adjuvants, defects after done curettage, recurrence, metastasis, fractures in post-operative, switching grade (from one grade to another grade), death, bone graft, tumor characteristics, survival rate, outcome, chemo and radiotherapy, metallic implants, and other diseases in these two tables mentioned. Was done the comparison with our hospital data among their literature information’s, because of getting more accurate comparison results to know more about current outcomes of chondrosarcoma.
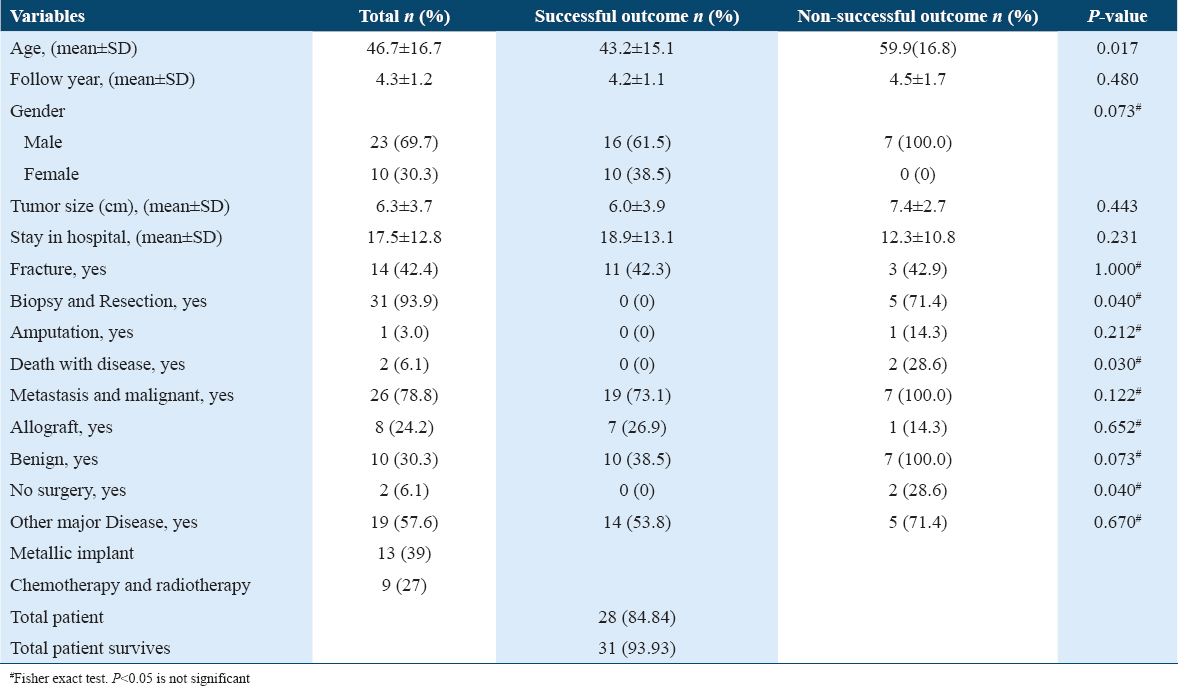
In Table 2, we are going to analyze our collected data from our hospital database. All tests here were two-sided, and P < 0.05 was considered significant. This series of the patient’s treated from 2013 and recorded in the hospital database. We found that 33 patients had Grade 1–3 types of chondrosarcoma. In this article, patients age range 16–79 years (46.7 + 16.7) and their follow-up years 4.3 + 1.2. Our patient’s male-female ratio is 23:10, where 69.7% of patients are male. As we know, chondrosarcoma affects males more than females. In 13 patients were tumors located in the humerus 13 (39.39%), 9 (27.27%) femur, 5 (15.15%) tibia, 4 (12.12%) pelvis, 2 (6.06%) scapula, and other areas such as Spine is 9 (27.27%). Out of 33 patients, 31 patients did the surgery, and two patients went to the oncology department to getting the chemotherapy cycle first. The patient’s tumor size is 6.3 + 3.7 cm. Our patients were staying in the hospital according to their chondrosarcoma grade (1–3), pre and post-surgical situations 17 + 12.8 days. 19 (57.56%) patients had other major diseases such as lung infections, bone tuberculosis, sciatica, herniation, degeneration, and a few of them had a surgical history as well. 14 patients had a fracture in different locations, which is 42.4% among all 33 patients. 23 patients had metastasis, which is 69.69%, and ten patients are in the benign stage of chondrosarcoma tumors. Hence, we can say most of the patients had I and II grade chondrosarcoma tumors. Our experts have done a biopsy for all of our patients. There is one patient who had an amputation to avoid recurrence and spread in other parts of the body. Two patients died after surgery within 2 years of follow-up. Eight (24.2%) patients had a bone graft, and 13 (39.39%) patients had metallic implants because of fractures that occurred due to lack of bone density. We also used bone cement in 5 (16%) cases out of 31. There are 13 (39%) patients whose surgeries were curettage. We have chosen wide resection for most patients, which are about 17 (54.83%) cases, marginal resection was 7 (21.21%), and intralesional resection was 2. We sent to our oncology department two patients for complete three cycle chemotherapy and suggested to do surgery after that. A total of 9 (27%) patients had chemotherapy and radiotherapy before or after surgery. Total death with the disease during follow-up years is 2 (6.1%), which is considerable because those two patients had Grade 3 chondrosarcoma. Our hospital’s total successful outcome is 28 (84.84%), because of their motion, the function was up to the mark (including metallic implants), and no chondrosarcoma recurrence occurred among them. The total survival rate, according to our follow-up years, was 31 (93.90%) patients.
Sensitivity analysis and publication bias
In the sensitivity analysis for the main indicators used differently for those studies whose selection bias is unclear due to the removal of the random sequence generation method, whether or not to apply intentionality analysis, the conclusion of the final data combination has not changed. The results are stable. Less than a few papers were included in each analysis, so there were no conditions for evaluating publication bias.
Discussion
We recognize that the diagnosis and treatment of these tumors have evolved with time, and some treatment of these lesions treated long ago might be treated differently today. The same primary tumor treated with an amputation during the early period of our study may be treated with wide excision today. Each of these techniques carries different risks and benefits. Although most of the chondrosarcoma grades (1, 2, and 3) and subtypes, surgical treatment offering only chances for recovery from the disease, it is still debated about the most optimal surgical management. If we consider morbidity and a demanding reconstruction, depending on the location followed by local adjuvant treatment, for example, liquid nitrogen/distilled water, and bone graft with wide resection can lead to promising long-term clinical outcomes. But using distilled water as an adjuvant during all surgical procedures show the better outcome, because of only 2 (6.1%) recurrence cases we have seen among all chondrosarcoma grade patients. In most of these cases, the preferred choice for our surgical treatment was remaining wide resection. As compared with all of the author’s literature, chondrosarcoma grade is 1 or low grade, although 20 (61%) patients from our data are Grade 2. Other regions author’s literature [Table 1 and 3], most of their patients are affected on limbs as same as our patients, which shows no differences. Total follow-up years of other author’s literature are slightly longer than us, but it is not changed these rare tumor cases result much. There are no defects noticed after curettage among our patients, but few patients, among other author’s literature [Tables 1 and 3], show there are defects. There is a very low (6.1%) recurrence after surgery among our patients, but most of the other authors [Tables 1 and 3] data shows that their patient’s tumor recurrences are one-third. Most of the authors mentioned that they use adjuvants, such as phenol, liquid nitrogen or cryoprobes, or H2O2 for surgery, but we are using distilled water only to protect recurrence, and the result is adequate with a reasonable survival rate of 94%. Few authors [Tables 1 and 3] data show there are post-operative fractures; on the other hand, there is no available data about in our study. Few authors [Tables 1 and 3] literature data show in the table that fewer is switch to a different grade of chondrosarcoma, wherein our data there is none. Table 1, we have a low rate amputation, but the higher rate in Mourikis et al. chondrosarcoma affects mostly males than females, but Mourikis et al. (n = 31) and Bindiganavile et al. (n = 125) literature shows that female is more than male. Our institution’s death rate with the disease is lower than Bindiganavile et al. than a Korean institution. Bindiganavile et al. data show low metastasis than Mourikis et al. and our data. Metallic implant, fracture, and a bone graft are a high rate in Mourikis et al. data than ours, on the other hand, there are no data about it in Bindiganavile et al. literature. In our institution, 27.27% of patients had taken chemo and radiotherapy, which is a very high rate than other author’s patient data. We have got 42% of patients who have another major disease, but there is no data available among other author’s literature. Total survival and successful outcome among our patients are 94% and 85%, which are better than the USA and Korean institutions [Table 1].
This study has a few limits. First, it is not a prospective study, but the rarity of this tumor and the need for extended clinical follow-up make it challenging. Second, comparison of different treatments was not randomized, but based on current information about this pathology; and third, the monitoring of our patients is significant, but still too short for considerations with outcomes.
Conclusion
After optimal diagnosis and treatment by an experienced team of specialists, although chondrosarcoma tumors generally have an excellent prognosis. Analysis of the difference between surgical technics and patient outcomes has been limited due to the sparseness of these lesions and few institutions having enough patients and data. Furthermore, different regions and institution’s surgical, clinical diagnosis, and treatment are slightly not similar. We observed that females are get affected more than males among those institutions’ chondrosarcoma patients, which is alarming somehow, because chondrosarcoma characteristics may be changing gradually around the globe. Although our study found that using distilled water as an adjuvant and wide resection giving significantly better results for Grades 1 and 2 chondrosarcoma treatments among our 33 patients than compared institutions patients, the total survival rate is 94% and a successful outcome is 85%. To get more accuracy and evidence of this result need to conduct further research on a clinical basis because of relatively short follow-up and non-randomized study limitations. This is a systematic review which is a relatively high level of generalizability due to the inclusion of patients among institutions and countries. It may also be susceptible to bias associated with individual patients being reported over others.
Authors’ Declaration Statements
Availability of data and material
On reasonable request, data portion will be available, but all data are not publicly available, because of patient’s information.
Funding statement
The authors received no financial support for the research or publication.
Authors’ Contributions
SAJ and SJ conceived and designed the study; SAJ, LCH, ZX, YW, and ZZ collected the data; SAJ and LCH checkout the follow-up; SAJ and LCH wrote different parts of the manuscript; SJ, ZX, and YW revised the manuscript. All authors approved the final manuscript.
References
- Chondrosarcoma in the United States (1973 to 2003):An analysis of 2890 cases from the SEER database. J Bone Joint Surg Am. 2009;91:1063-72.
- [Google Scholar]
- Prosthetic replacement of the proximal humerus. Clin Orthop Relat Res. 1987;224:178-91.
- [Google Scholar]
- Chondrosarcoma of bone. The experience at the istituto ortopedico rizzoli. J Bone Joint Surg Am. 1981;63:1248-57.
- [Google Scholar]
- Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br. 2005;87:1527-30.
- [Google Scholar]
- Chondrosarcoma:Clear-cell variant. A report of sixteen cases. J Bone Joint Surg Am. 1976;58:676-83.
- [Google Scholar]
- BONE TUMORS. Howard D. Dorfman and bogdan czerniak. St. Louis, Mosby, 1998. $225.00, 1261 pp. J Bone Joint Surg. 1999;81:899.
- [Google Scholar]
- Chondrosarcoma in Norway 1990-2013;an epidemiological and prognostic observational study of a complete national cohort. Acta Oncol. 2019;58:273-82.
- [Google Scholar]
- Mega Tumour (chondrosarcoma) of humerus-an insanely large tumor and its social implications. J Orthop Case Rep. 2017;7:102-5.
- [Google Scholar]
- Chondrosarcoma of bone:An assessment of outcome. J Bone Joint Surg Am. 1999;81:326-38.
- [Google Scholar]
- Relationship between surgical procedure and outcome for patients with grade I chondrosarcomas. Clinics (Sao Paulo, Brazil). 2005;60:121-6.
- [Google Scholar]
- Grade I chondrosarcoma of bone:The Munster experience. J Cancer Res Clin Oncol. 2009;135:543-50.
- [Google Scholar]
- Chondrosarcoma of the scapula:Long-term oncologic outcome. Cancer. 2005;104:149-58.
- [Google Scholar]
- Prognostic factors in chondrosarcoma of bone:A clinicopathologic analysis with emphasis on histologic grading. Cancer. 1977;40:818-31.
- [Google Scholar]
- A system of staging musculoskeletal neoplasms. Clin Orthop Relat Res. 1986;204:9-24.
- [Google Scholar]
- Effect of distilled water on rapid inactivation of tumour cells attached to surgery instruments. Int J Nurs Pract. 2014;20:524-9.
- [Google Scholar]
- Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res. 2002;397:19-28.
- [Google Scholar]
- Radiofrequency ablation therapy combined with cementoplasty for painful bone metastases:Initial experience. Cardiovasc Intervent Radiol. 2005;28:578-83.
- [Google Scholar]
- Clinical assessment of percutaneous radiofrequency ablation for painful metastatic bone tumors. Cardiovasc Intervent Radiol. 2006;29:1022-6.
- [Google Scholar]
- Low-grade chondrosarcoma of long bones treated with intralesional curettage followed by application of phenol, ethanol, and bone-grafting. J Bone Joint Surg Am. 2012;94:1201-7.
- [Google Scholar]
- Low-grade chondrosarcoma of bone:Experiences from the vienna bone and soft tissue tumour registry. Int Orthop. 2011;35:1049-56.
- [Google Scholar]
- Survival and prognostic factors in chondrosarcoma:Results in 115 patients with long-term follow-up. Acta Orthop. 2011;82:749-55.
- [Google Scholar]
- Surgical treatment of grade I central chondrosarcoma. Clin Orthop Relat Res. 2010;468:581-9.
- [Google Scholar]
- Curettage and cryosurgery for low-grade cartilage tumors is associated with low recurrence and high function. Clin Orthop Relat Res. 2010;468:2765-73.
- [Google Scholar]
- No recurrences in selected patients after curettage with cryotherapy for grade I chondrosarcomas. Clin Orthop Relat Res. 2010;468:1956-62.
- [Google Scholar]
- Extended intralesional treatment versus resection of low-grade chondrosarcomas. Clin Orthop Relat Res. 2009;467:2105-11.
- [Google Scholar]
- Outcome of intralesional curettage for low-grade chondrosarcoma of long bones. Eur J Surg Oncol. 2009;35:1343-7.
- [Google Scholar]
- Oncological and functional results of cryosurgical therapy of enchondromas and chondrosarcomas grade 1. J Surg Oncol. 2008;98:421-6.
- [Google Scholar]
- Surgical management of conventional grade I chondrosarcoma of long bones. Clin Orthop Relat Res. 2007;463:166-72.
- [Google Scholar]
- Influence of cryosurgery on treatment outcome of low-grade chondrosarcoma. Clin Orthop Relat Res. 2006;451:201-7.
- [Google Scholar]
- Treatment of proximal humeral chondrosarcoma with resection and allograft. J Shoulder Elbow Surg. 2007;16:519-24.
- [Google Scholar]
- Long-term outcome of chondrosarcoma:A single institutional experience. Cancer Res Treat. 2015;47:897-903.
- [Google Scholar]




