
Translate this page into:
Developing an attitude toward polio vaccination scale and establishing its psychometric properties in Pakistani context for indigenous and international researchers
Address for correspondence: Muhammad Kamran, Department of Education, University of Loralai, Balochistan, Pakistan. Phone: +92-344-9370970. E-mail: muhammad.kamran@uoli.edu.pk/kamrankundi86@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Qassim Uninversity and was migrated to Scientific Scholar after the change of Publisher.
Abstract
ABSTRACT
Objectives:
Negative attitudes toward polio vaccination in Pakistan are threatening the global polio eradication efforts by encouraging vaccine refusals and attacks on polio workers. The present research explored the underlying dimensions of these attitudes and their correlates: Uncertainty and belief in conspiracy theories.
Methods:
This research began with the development of an item pool generated with the help of an open-ended survey of university students (n = 44). Face and content validity assessment by subject experts (n = 9) led to an initial version of the attitude toward polio vaccination scale (ATPVS). This scale was administered to a sample of Pakistani adults (n = 620) through two means: Paper-and-pencil survey and an online survey.
Results:
Exploratory factor analysis on one-half of the sample (n = 310) suggested a factor structure consisting of two internally consistent factors: Scepticism and Advocacy. On second half of the sample (n = 310), confirmatory factor analysis confirmed the two-factor structure of this scale. Hypothesis testing for convergent validity on the total sample (n = 620) revealed that self-uncertainty was positively related to scepticism and negatively related to advocacy. Whereas conspiracy mentality was positively associated with both of these components which indicates an understudied aspect of this construct related to concern for social welfare.
Conclusion:
Scepticism and advocacy of the polio vaccination campaign represent attitudes toward polio vaccination in Pakistan with self-uncertainty and conspiracy mentality being their significant correlates. Capitalizing on these variables in designing a vaccination promotion campaign may yield benefits.
Keywords
Attitude toward polio vaccination
conspiracy mentality
conspiracy theories
polio vaccines
polio
self-uncertainty

Introduction
The persistence of poliovirus in Pakistan is undermining the efforts of the Global Polio Eradication Initiative.[1] Significant barriers responsible for the persistence of polio in Pakistan are vaccine hesitancy and refusals by parents.[2,3] Vaccine refusals by families were responsible for 40% of the Wild Polio Virus cases occurring in 2014.[4] Negative attitudes toward polio vaccines are not only driving these refusals[5] but they are also leading to violent attacks on polio workers.[6]
An incident in 2019 demonstrates the risk posed by anti-polio vaccination attitudes in Pakistan. In the Khyber Pakhtunkhwa (KPK) province, an angry mob burnt down a healthcare unit after a viral hoax stating that children were rushed to hospital with various medical complaints following polio vaccination.[7] Such serious implications underscore the need for assessing vaccine related attitudes. Empirical assessment of vaccine related attitudes can also help in predicting the likelihood of getting vaccinated because attitudes exert influence on behavior.[8] In the long run, this assessment can facilitate the development of more tailored eradication interventions.[5]
The first step in this endeavor requires the utilization of a psychometrically sound instrument for measuring attitudes toward polio vaccination as they exist in Pakistan. There are three similar measures of attitude toward polio immunization available.[5,9,10] However, the internal reliabilities of these instruments are low to moderate and they have been developed for specific samples (i.e., health workers, religious scholars, and residents of Quetta/Peshawar). The validation procedures for these scales only involved expert reviews and try-outs with small samples.
There are also several measures[11,12] for measuring general vaccination attitudes. However, the tool measuring attitudes toward polio vaccination can benefit from being more indigenized as these attitudes are shaped by the unique socio-political context of Pakistan.[13] The nature of this particular context has been explored by previous studies.
Polio vaccine refusals in Pakistanis, more specifically, Pakhtuns were significantly increased when the U.S. killed Osama bin Laden, the former Al-Qaeda chief, in a military operation in Pakistan by reportedly using a fake hepatitis vaccination campaign to trace bin Laden.[13] These refusals have been more prevalent among ethnic groups that inhabit regions like KPK and Balochistan, where conflict and insecurity is common.[3] These conditions exacerbate uncertainty which can stem from the immediate situation or the overall social environment.[14]
People perceive getting vaccinated to be riskier than not getting vaccinated under conditions of uncertainty.[15] Uncertainty about vaccination itself can lead to vaccine hesitancy and mistrust.[16] Furthermore, uncertainty about one aspect of life can influence other types of uncertainty.[17] Therefore, it is expected that such uncertainties influence self-uncertainty-uncertainty about one’s attitudes, beliefs, values, and place in the world which produces such aversive feelings that one is motivated to reduce them.[17]
One way of reducing self-uncertainty is becoming attached to a group or group identification,[18] a process which makes extremist propaganda more persuasive[19] and increases beliefs in conspiracy theories because people are only worried about conspiracy theories when their group identification is strong and they fear hostility from another group.[20] Conspiracy theories on their own can combat uncertainty by giving meaning to events beyond comprehension.[21] This is evidenced by the fact that people, throughout history, have shown more belief in conspiracy theories during times of conflict and crises like natural disasters, societal change, and wars.[22] Thus, it is likely that anti-vaccination conspiracy theories become more persuasive under conditions of uncertainty. This assumption holds serious implications for the polio vaccination campaign in Pakistan, a country where the tendency to believe in general conspiracy theories is prevalent.[23]
This general tendency to believe in conspiracy theories significantly increases anti-vaccination attitudes.[24] Belief in specific anti-vaccination theories also predicts anti-vaccination attitudes.[25] Since belief in specific conspiracy theories depends on the general tendency to hold such views[26] - a general conspiracy mentality.[27] Hence, it can be predicted that a conspiracy mentality negatively influences attitudes toward polio vaccination.
In Pakistan, anti-vaccination propaganda widely spreads through social media[28] and poses a significant hurdle in the eradication of polio by peddling various conspiracy theories.[13] These conspiracy theories are usually about the content, efficacy, and harmful effects of the polio vaccine[2,29,30] such as rumors that the vaccine contains pig fat, which Muslims are forbidden to consume, or that, polio vaccines cause infertility.
Statically testing the links of these variables with attitudes towards polio vaccination can help form efficacious intervention designs. However, to the best of the author’s knowledge, almost all studies about polio vaccination attitudes in Pakistan have been qualitative or descriptive.[1,2,5,30-34] Another avenue worth exploring is the difference between attitudes of men and women toward polio vaccination because these studies have not been able to find significant gender differences.[5]
Due to the significance of attitudes toward polio vaccination and the paucity of research on their psychological influencers, the present research has taken the initiative of exploring the dimensions of these attitudes. This research aims to develop an attitude toward polio vaccination scale (ATPVS) and establish its psychometric properties. Due to evidence of their link with attitudes toward vaccination uncertainty and conspiracy mentality have been explored as correlates and indicators of convergent validity.
Methods
The research commenced after approval was granted by the ethical review committee (IRB: F.No.D-107-02(02)M.Phil/Fall-2018-Admin Permission granted December 11, 2019) at the National Institute of Psychology, Quaid i Azam University, Islamabad, Pakistan. The development of ATPVS was undertaken in two phases; phase 1 was about scale development and phase 2 consisted of scale validation procedures including exploratory factor analysis (EFA), confirmatory factor analysis (CFA), and testing of convergent validity.
Phase 1: Scale development
This study was aimed at developing ATPVS and establishing its psychometric properties. It consisted of four phases that involved creation of an item pool as well as establishment of face and content validity.
Step I: Creation of an item pool
To generate items for ATPVS, an open-ended survey was conducted. Through convenient sampling, 44 students were recruited from different public universities in Rawalpindi and Islamabad. This sample comprised of female (n = 25) and male (n = 19) students within the age range of 18–27. These students belonged to Punjab (n = 17), KPK (n = 12), Balochistan (n = 5), and Sindh (n = 4) provinces of Pakistan. The reason for selecting public university students for this open-ended survey was that they tend to have diverse cultural, ethnic, and socioeconomic backgrounds. Therefore, the recruitment of students from government universities proved to be advantageous in conveniently procuring a diverse group representing main regions of Pakistan. As opinions about polio vaccines differ across provinces of Pakistan[28] so diversity of samples in this phase helped in gathering more varied views about polio vaccination.
Four open-ended questions, inspired by the previous research[2,33,34] gauged participants’ opinions about polio vaccination in general, perception of the seriousness of polio, repeated vaccine administrations, and general concerns. These questions were posed in English and Urdu. Participants preferred to write their responses in English which could because English is the most commonly used language of instruction in the higher education sector of Pakistan.[35]
A content analysis of their responses generated the wider themes of belief in the seriousness of polio, vaccine safety, vaccine efficacy, vaccine advocacy, and conspiracy beliefs about polio vaccines, which were converted into statements later. Other themes generated from this survey matched items of existing measures so eight items from three versions of attitude towards polio immunization scale[5,9,10] were modified and added with the author’s permission. Finally, an item pool containing 30 items was formed. All the items were in English.
Step II: Establishing content validity
Nine Subject Matter Experts (SMEs), who held experience in research and scale development, evaluated the face validity, construct relevance, and clarity of the 30 items. In addition, the content validity of items was assessed by calculating Content validity ratios (CVR). The CVRs for most items were above the acceptable limit of 0.78 which is the minimum value of CVR for nine panellists required for establishing content validity.[36] Since the CVRs for items 4 and 11 were below this value, they were discarded from the scale. After incorporating suggested modifications, an initial version of the ATPVS, containing 28 items, was formulated.
Phase II: Validation
After finalization of items, a number of validation procedures were performed to establish the psychometric properties of the ATPVS. These procedures included conducting an item-to-total correlation analysis, EFA, CFA, reliability estimation, and establishment of construct validity.
Sample
In this phase, the total sample consisted of 620 Pakistani adults. Sample size was estimated with the goal of conducting exploratory and confirmatory factor analyses in mind. Recommendations about sample selection for EFA suggest that sample size should be at least 10 times greater than the total number of items.[37] Similarly, in case of CFA, an accepted ratio is also 10 cases per variable.[38] Since there are 22 items in ATPVS, therefore the desired sample size was estimated to be at least 220 per each analysis or 440 in total.
The targeted sample for this research was the Pakistani adult population. The inclusion criteria for their participation were set at a minimum education level of 12 years and minimum age of 18 years. This particular criterion was set to ensure sufficient understanding of the English language so participants would not face difficulty in comprehending ATPVS. English proficiency was also mentioned as a criterion for participation in the informed consent of the survey.
Convenient method of sampling was used to collect data in two ways: in person and online. In-person data were collected from university students of Islamabad and Rawalpindi. A total of 350 of questionnaires were distributed in field. Data of 310 respondents were retained and the rest was discarded owing to incomplete responses that exceeded more than 5% missing values on ATPVS. Due to the emergence of COVID-19 epidemic, in person data could not be collected further.
Online data were collected through a survey hosted on Stoet and Psytoolkit.[39,40] A total of 855 adults viewed the survey out of which 543 people participated. However, only 310 complete responses were retained because rest of the forms were left more than 5% incomplete. Final count of retained responses stood at 620 consisting of both online and in person data.
There were 214 (34.6%) men and 405 (65.4%) women in the final sample. Their age ranged from 18 to 91 (M = 23.10, Standard deviation = 7.17). Province-wise, 411 (66.3%) participants were from Punjab, 100 (16.1%) from Federal Areas, 53 (8.5%) from KPK, 11 (1.8%) from Azad Jammu and Kashmir, 7 (1.1%) from Sindh, and 6 (0.96%) from Baluchistan. Among the sample, 350 (56.4%) responded that children in their family were receiving polio vaccines, while, 156 (25.22%) indicated that children in their family were not receiving vaccines.
Instruments
The description of instruments used in this research for establishing construct validity is given below:
Initial form of ATPVS
To determine attitudes toward polio vaccination, a 28-item English language measure developed in Phase I of this research was utilized. It was a six-point scale with following response options: 1= strongly disagree, 2 = disagree, 3 = slightly disagree, 4 = slightly agree, 5 = agree, and 6 = strongly agree.
Self-uncertainty scale
A 12-item self-uncertainty scale α = 0.89 was used to measure participants’ feelings of self-uncertainty about self, world, and future.[41] It was rated on a 7-point scale (1 = Disagree strongly to 7 = Agree strongly). Questions 6 and 11 were reverse-recoded so that higher scores indicated greater self-uncertainty.
Conspiracy mentality questionnaire (CMQ)
The five-item measure (a = 0.82) was used to assess participants’ conspiracy mentality. It consisted of general statements capturing a conspiracist view of world events.[42] Participants indicated on 11-point scales how likely they thought each item to be true from 0 (0%– certainly not) to 10 (100%-certain). The minimum score that could be obtained on this scale was five while the maximum was 50. High scores on this scale indicated a greater tendency to believe in conspiracy theories.
Data collection process
The process of data collection began in December 2019. Prospective participants were approached in the universities of Islamabad and Rawalpindi. Willing participants received hard copies of the questionnaire. The purpose of the research, its associated risks and benefits, and rights of confidentiality as well as anonymity were conveyed to them orally and through written informed consent. Participants were encouraged to participate by informing them how their responses will add to the understanding of polio’s persistence in Pakistan. Participants then gave their signatures to indicate their willingness to participate. At the end of the survey, participants gave their feedback and were thanked for their participation.
Further data collection was halted by the advent of COVID-19 pandemic in March. Resultant suspension of on-ground academic activities in Pakistan,[43] led to a modification in the data collection strategy. Remaining data collection proceeded through an online survey hosted on Stoet and Psytoolkit.[39,40] The survey linked was shared to prospective participants through WhatsApp. A detailed informed consent listing the purpose of the survey, eligibility criteria for participation, benefits of participation, voluntary nature of participation, rights of confidentiality, and rights of data protection, was provided to participants in the welcome screen. Participants also had the option to view their automatically calculated scores on attitude toward polio vaccination at the end of the survey. The duration of data collection lasted for almost a month.
At end of the data collection process, the sample size stood at 620 including in-person and online data. This data were split into two groups along the basis of the two mediums used to collect data. Data from the first group consisting of university students were used to conduct EFA for ATPVS. The second group, consisting of a more diverse sample of Pakistani adults collected online was used to test the validity of ATPVS on an independent sample.
Before carrying out further psychometric analyses, missing values of ATPVS items that possessed >5% missing values[44] were imputed using series mean substitution. SPSS version 21 was used to conduct various statistical analyses involved in this phase.
Results
This section contains results of various validation procedures carried out for the ATPVS.
Item-to-total correlation
For the purpose of establishing the construct validity of the ATPVS, item-to-total correlations were computed for the first half of the sample containing 310 participants. Pearson Product Moment Correlation analysis was used to analyze 28 items. Item-to-total correlations for all items were significant except for items 2 and 12. Thus, a decision was made to discard these two items.
EFA
Further analysis was completed on the remaining 26 items to determine the underlying dimensions by means of EFA. First half of the sample was used for this analysis. Initially, the Kaiser-Meyers-Olkin (KMO) measure of sampling adequacy and Bartlett’s Test of Sphericity were computed to check the sampling adequacy (n = 310). KMO = 0.83 illustrated that correlations were compact enough to generate distinct and reliable factors with Bartlett test of Sphericity χ² (325) = 2120.73 significant at P < 0.001 showing that the data was good enough for carrying out EFA. After the convergence of factor solution in 50 iterations, seven factors with Eigenvalues <1 were suggested. Since these seven factors were neither comprehensive nor interpretable, the Varimax method of rotation was used for the purpose of extracting meaningful factors. Subsequently, three more factor structures consisting of 2, 3, and 4 factors were extracted. SMEs were recruited to assess the meaningfulness of all these factor structures.
The 4-factor solution was discarded after the consensus of the majority of SMEs (n = 7) around 2 and 3-factor structures being more meaningful. Upon testing the alpha reliabilities of the three factors, reliability coefficients turned out to be 0.84, 0.74, and 0.40. Weak alpha value of the third factor did not improve even after omitting a few items. Therefore, the three-factor solution was also discarded. Finally, a two-factor solution was tested whose factor loadings are presented in Table 1.
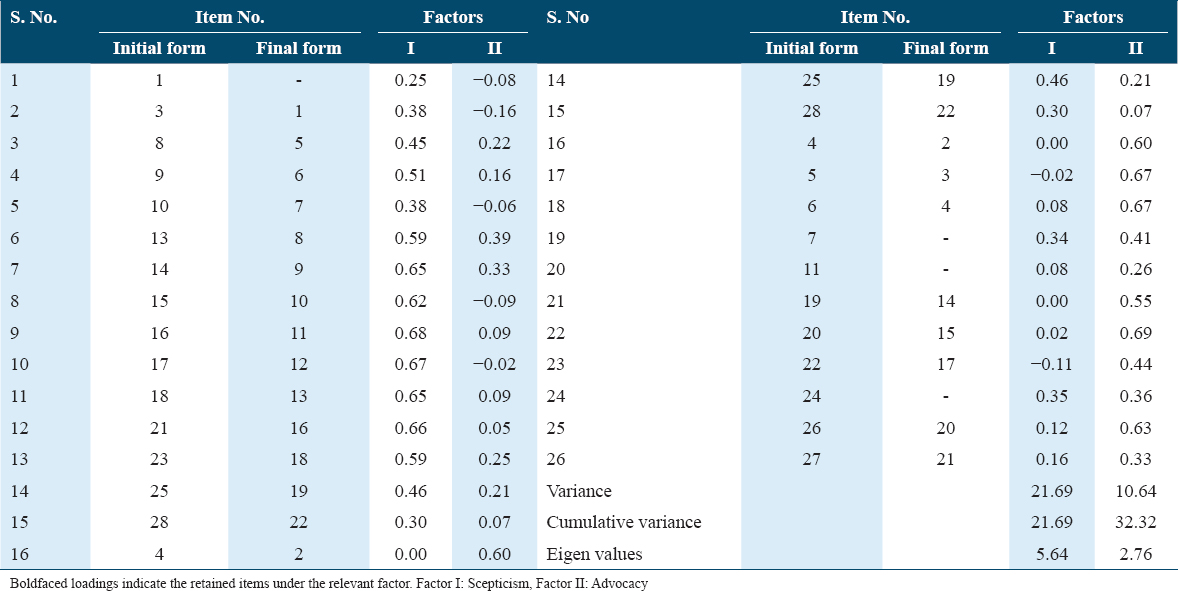
In the two-factor solution presented in Table 1, only items that had factor loadings of 0.30 were retained because an item loading of about 0.30 or more is considered significant for a sample size similar to the present study.[45] Items 1 and 11 were discarded for having low factor loadings. Whereas, items 7 and 24 were discarded for cross-loading on both factors I and II. The final solution containing Factor I and Factor II were not only qualitatively meaningful, but the alpha coefficients of the two factors were above 0.70.
The ATPVS consisting of 22 items was finalized as consisting of two dimensions or factors. Factor I was named Scepticism while Factor II was named Advocacy, as per the suggestion of SMEs. Items of Scepticism reflected doubts about the safety of polio vaccines, concern about their harmful effects, and belief in conspiracy theories about polio vaccines. Items of Advocacy indicated belief in the effectiveness of polio vaccines and support for the vaccination campaign. Reliability analysis revealed alpha coefficients of 0.83 and 0.73 for Scepticism and Advocacy, respectively. The inter-subscale correlation value showed a significant association of −0.27 between the two factors.
Confirming the factor structure of ATPVS
To assess the psychometric meaningfulness of two factors of ATPVS and to test its validity for use with a heterogeneous sample, the second half of the sample, containing 310 adult participants was used. AMOS 22 statistical package was used to conduct CFA with maximum likelihood. The various model fit indices computed to evaluate this model are presented in Table 2.

Initially in the default model, hypothesized CFA for ATPVS yielded unsatisfactory model fit indices. For a model to be considered acceptable, the NFI, GFI, and CFI should be <0.90, 0.90, and 0.93 respectively.[46] Whereas, the RMSEA value should be >0.08[47] and χ²/df value should be >2 or 3.[48] To improve these indices, error covariance’s were drawn between all possible error terms suggested by modification indices [Figure 1].
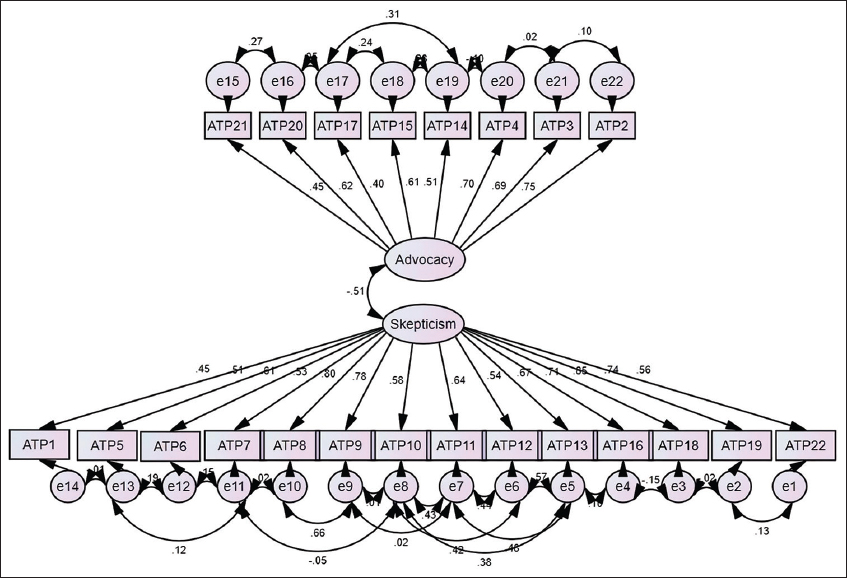
- Measurement model of ATPVS
After adding these error covariance’s, all model indices fell within the acceptable range except for NFI. The standardized factor loadings for Scepticism and Advocacy are given in Table 3.
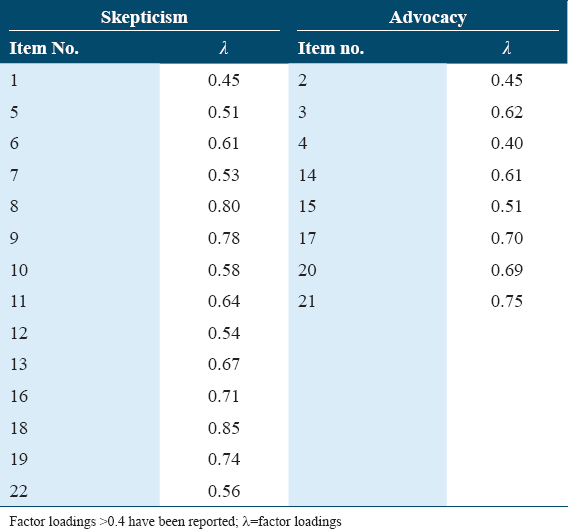
It is evident from Table 3 that all items possess acceptable factor loadings, that is, >0.40,[49] on the two subscales of ATPVS, Scepticism, and Advocacy. Thus, the factor structure of ATPVS, as proposed by EFA, has been confirmed through a CFA on an independent sample. Furthermore, Cronbach’s alphas of Scepticism and Advocacy calculated for this sample showed α-values of 0.91 and 0.82, respectively.
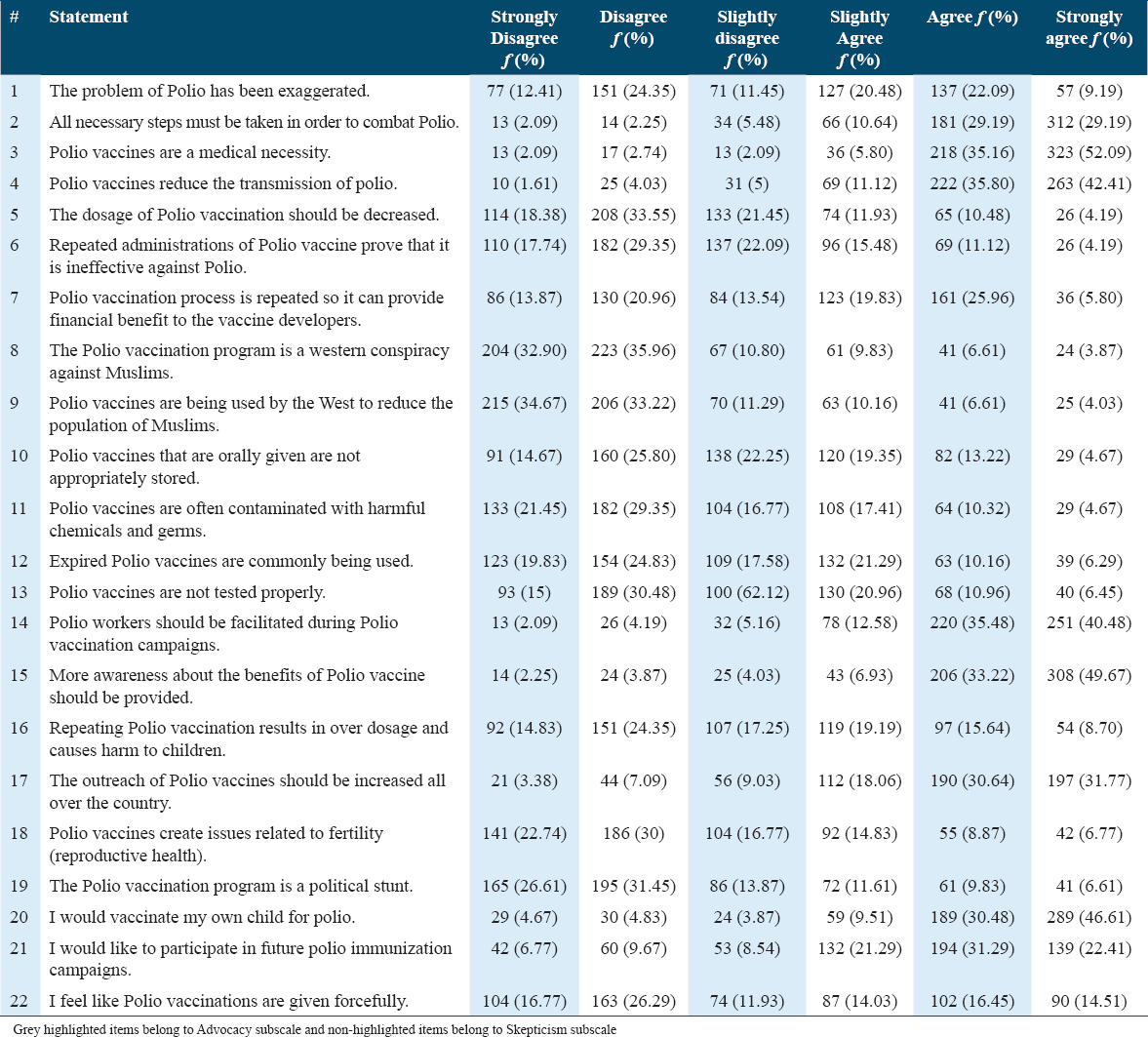
Frequency analysis for ATPVS items
The data of the total rom two previous samples (i.e., on-field and online) were combined for frequency analysis of responses to ATPVS [Table 4]. This data of 620 individuals consists of Pakistani adults who possess English literacy.
Convergent validity
Pearson Product Moment was used to assess the links of self-uncertainty, conspiracy mentality, and the two components of attitude toward polio vaccination, scepticism, and advocacy. The correlations coefficients of these variables along with the descriptive properties and alpha reliabilities for their measures have been tabulated [Table 5].

The correlation matrix suggests that scepticism and advocacy have a significantly negative relationship between themselves. Conspiracy mentality has a positively significant relationship with both components of ATPVS; therefore, an increase in conspiracy mentality is associated with increases in both scepticism and advocacy of polio vaccination. Moreover, increase in self-uncertainty is associated with an increase in scepticism and a decrease in advocacy.
Gender Differences in attitudes towards polio vaccination
Independent-sample t-test was utilized to assess gender differences in attitude towards polio vaccination, self-uncertainty, and conspiracy mentality [Table 6].

It is evident that gender differences in attitude toward polio vaccination are present but with a small effect size.[44] Women are showing less scepticism and more advocacy of polio vaccination as compared to men as evident from the group mean scores.
Discussion
There is a dearth of instruments that adequately address attitudes towards polio vaccination. Therefore, this research took the initiative of developing ATPVS to accurately reflect indigenous attitudes toward polio vaccination. An EFA and a subsequent CFA resulted in the most significant finding of this research: Attitudes toward polio vaccination in Pakistan are reflected by two dimensions; skepticism and advocacy. Skepticism covers doubts about the safety of polio vaccines, concern about their harmful effects, and belief in conspiracy theories about polio vaccines. Such concerns have also been identified by previous studies (Closser et al. 2015; Khan et al. 2020).[2,31]
The factor, advocacy, covers support for the vaccination campaign. This aspect is unique in the sense that it covers advocacy of polio vaccination on a country-wide level (e.g., ”polio workers should be facilitated during polio vaccination campaigns” and “outreach of polio vaccines should be increased all over the country). This reflects the social welfare aspect of vaccination[52] something that goes beyond personal concern. Thus, an effective campaign can benefit from a two-pronged approach: Tackling misinformation about polio vaccination and appealing to concern for social welfare.
Next, it was observed through a frequency analysis of responses to ATPVS by the combined sample that most participants tended to agree with items of the advocacy subscale, thereby, indicating their support for polio vaccination campaign and their willingness to participate in it. This finding could have occurred due to certain sample characteristics – being young, single and mostly hailing from Punjab – associated with positive attitudes towards polio vaccination.[51]
For the Skepticism scale, it was observed that participants disagreed with statements of most items, thereby, indicating their positive attitudes. However, participants showed agreement to two items: Item 1 that states that the problem of polio has been exaggerated, item 7 that states that the vaccine process is repeated so it can provide financial benefit to the vaccine developers. This finding provides proof for the two-factor structure of ATPVS in which skepticism and advocacy are not simply opposite constructs. Thus, participants who might be showing more advocacy of polio vaccination can also hold certain skeptical attitudes. However, it is also likely that these two items may be representing factual statements that individuals might be agreeing with, irrespective of their positive attitudes. Further analyses of these items are required to confirm this possibility. Nevertheless, even a few such doubts can indicate vaccine hesitancy which can soon turn into refusals.[52] Vaccine refusals from even a few individuals can result in the emergence of unvaccinated clusters where a disease outbreak might occur.[53]
Converge validity was established by exploring the relationship of ATPVS with Self-Uncertainty Scale[41] and CMQ.[42] Results revealed that self-uncertainty was positively related with skepticism and negatively related with advocacy, thereby, supporting the hypothesis that uncertainty is associated with negative vaccination attitudes. It should be noted that self-uncertainty can bleed into other uncertainties and vice-versa.[17] Hence, if uncertainty related to vaccination can lead to vaccine hesitancy and mistrust[17] then self-uncertainty is likely to have a negative effect as well. The findings of this study regarding self-uncertainty are also in line with the proposition that uncertainty can strengthen belief in conspiracy theories.[20]
The need to assess vaccine decision-making in the presence of uncertainty has significant implications for Pakistan because uncertainty prevails in low-income emerging economies[54] and this need has now become even more salient in the conditions where global uncertainty is at record high levels due to Coronavirus.[55]
Next, results reveal that conspiracy mentality is associated with an increase in skepticism. This finding is in line with the hypothesis linking beliefs in conspiracy theories and anti-vaccination attitudes.[24,25,56] This construct holds implications for vaccination attitudes in general and also for polio vaccines. Negative propaganda regularly spreads online and promotes conspiracy theories[13] which often lead to mass panic[57] and acts of violence.[34] However, dealing with individual characteristics that make people susceptible to negative attitudes should be a greater priority for the government than curbing few factions peddling anti-polio vaccination propaganda.[58]
Coming to advocacy, its positive relationship with conspiracy mentality seems to go against the hypothesis that conspiracy mentality is associated with negative attitudes. However, there are arguments that conspiracy theories are not always associated with negative outcomes.[21] For example, conspiracy theories encourage protest movements[27] and bolster support for democratic principles.[59] This tendency also represents a desire to challenge the status quo to in turn seek truth and social advancement.[60] This social concern is already linked with decision-making about vaccines.[50]
Finally, it has been observed that women show more advocacy and less skepticism towards polio vaccination as compared to men. These small but significant gender differences in attitudes negate previous findings which found no significant gender differences in attitude towards polio immunization.[5] Future studies should recruit a more diverse sample with the help of translated instruments to discover more differences not just along the lines of gender but also demographics such as provincial background, marital status, and socio-economic level.
Strengths and limitations
Some strong points of the present study are highlighted in this section. Many items of both these factors cover issues that were not represented in existing instruments about polio vaccination.[5,9,10] The most significant advantage ATPVS holds over these existing instruments is the stringent validation process the scale has gone through.
The satisfactory results of almost all validation procedures suggest that ATPVS has displayed sufficient psychometric properties and can be used as a valid and reliable measure of attitudes towards polio vaccination across Pakistan. For instance, descriptive cross-sectional surveys can utilize ATPVS to gain a more psychometrically sound assessment of attitudes across different regions of Pakistan. The attitude differences observed through the use of this instrument can help identify groups where negative attitudes are prevalent so they can be targeted for interventions. Such data can help inform vaccination policies as a detailed understanding of people’s attitudes and opinions can lead to more effective health promotion practices.[61]
Furthermore, ATPVS also be used in Afghanistan, a country that forms a common epidemiological block with Pakistan.[62] Afghanistan borders Pakistan’s Khyber-Pakhtunkhwa and Northern Balochistan regions with majority of its population being Pashtuns.[63] It is worth mentioning that polio vaccine refusals are disproportionately reported from members of Pashtun ethnicity.[28] Hence, the exploration of ethnicity with polio vaccine refusals is another avenue where this instrument can be utilized. However, the development of instrument in English limits its use in assessing attitudes of more diverse samples. Hence, translation of this instrument can be taken up in future studies.
Future validation studies can help in refining ATPVS. One limitation was highlighted by the error covariances between adjacent items in CFA model [Figure 1]. High error covariances can result from adjacent placements of items on a questionnaire. Therefore, online administration of ATPVS can be advantageous in a sense that items can be presented to participants in a random order. Another issue exists with the similar wording of item 8 and 9 [Table 4]. This codependency is also evident by similar responses of participants to both of these items. Stringent validation studies can identify whether one of these items can be discarded or modified so it can address a different aspect of the stated conspiracy theory.
Another limitation of the study is the use of the CMQ.[42] This questionnaire has some issues with its construct validity as some items may be measuring the correctness of factual statement.[64] An indigenous instrument for conspiracy mentality that measures belief in conspiracies specific to Pakistan can be an alternative. Still, the positive role of conspiracy mentality with regards to vaccination attitudes needs to be explored in future studies.
The conclusions about the relationship among vaccination attitudes, conspiracy mentality, and self-uncertainty are limited by the cross-sectional nature of the study. Therefore, there is a need to conduct an experimental study to conclusively establish the predictive impact of self-uncertainty and conspiracy mentality on attitudes towards polio vaccination. Future studies can use an uncertainty prime[65] and manipulate conspiracy beliefs to reveal the meditational relationship of these three variables.
Conclusion
The present research has discovered underlying dimensions of attitudes toward polio vaccination and has led to the development of a psychometrically sound instrument called the ATPVS with its two subscales: Scepticism and advocacy. Self-uncertainty and conspiracy mentality have been established as correlates of these factors. The insight gained from this study can help in identifying individuals and contexts that increase susceptibility to anti-polio vaccination propaganda. In the long run, more individualized campaigns can be designed and implemented to help in achieving the complete eradication of polio from Pakistan.
Authors’ Contributions
WA, HJ, MK, and GMK were responsible for composing the manuscript; WA and HJ were responsible for conceptualizing the research question, data collection, and statistical analysis. WA, HJ, MK, and GMK also edited and reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Ethics Approval and Consent to Participate
All procedures carried out in this study were approved by the ethical committee at the National Institute of Psychology, Quaid-i-Azam University, Islamabad (IRB Number: F.No.D-107-02(02)M.Phil./Fall-2018-Admin Permission granted December 11, 2019). Written informed consents were taken from all participants.
Availability of Data and Material
The data that support the findings of this study will be provided by the corresponding author upon reasonable request.
Consent for Publication
All authors of this study gave their consent for publication.
Competing Interest
The authors declare they do not have any conflict of interest.
Funding Statement
No funding was provided for this research.
References
- Threats to polio eradication in high-conflict areas in Pakistan and Nigeria:A polling study of caregivers of children younger than 5 years. Lancet Infect Dis. 2015;15:1183-92.
- [Google Scholar]
- Polio eradication and health systems in Karachi:Vaccine refusals in context. Glob Health Commun. 2015;1:32-40.
- [Google Scholar]
- Eradicating polio in Pakistan:An analysis of the challenges and solutions to this security and health issue. Global Health. 2016;12:63.
- [Google Scholar]
- Global Polio Eradication Initiative (GPEI) Annual Report 2015. 2016. World Health Organization. Available from: https://polioeradication.org/wp-content/uploads/2016/07/2.2_12IMB.pdf
- [Google Scholar]
- Knowledge, attitudes and perceptions towards polio immunization among residents of two highly affected regions of Pakistan. BMC Public Health. 2015;15:1100.
- [Google Scholar]
- In:Pakistan, Polio Makes a Comeback Amid Vaccine Boycotts. 2019. Aljazeera. Available from: https://www.aljazeera.com/indepth/features/pakistan-polio-comeback-vaccine-boycotts-191226142838246.html
- [Google Scholar]
- A historical view on attitudes and persuasion. In: In:Oxford Research Encyclopedia of Psychology. USA: Oxford University Press; 2019. p. :1-34.
- [Google Scholar]
- A cross-sectional survey of healthcare workers on the knowledge and attitudes towards polio vaccination in Pakistan. PLoS One. 2015;10:e0142485.
- [Google Scholar]
- Muslim scholars'knowledge, attitudes and perceived barriers towards polio immunization in Pakistan. J Relig Health. 2017;56:635-48.
- [Google Scholar]
- Measuring vaccine confidence:Introducing a global vaccine confidence index. PLoSCurr. 2015;7:e033245.
- [Google Scholar]
- The vaccine hesitancy scale:Psychometric properties and validation. Vaccine. 2018;36:660-7.
- [Google Scholar]
- This is a Pakhtun disease:Pakhtun health journalists'perceptions of the barriers and facilitators to polio vaccine acceptance among the high-risk Pakhtun community in Pakistan. Vaccine. 2019;37:3694-703.
- [Google Scholar]
- Self-uncertainty and responsiveness to procedural justice. J Exp Soc Psychol. 2005;41:157-73.
- [Google Scholar]
- Attitudes to risk taking in medical decision making among British, Dutch and Belgian general practitioners. Br J Gen Pract. 1990;40:134-6.
- [Google Scholar]
- Vaccine hesitancy:In search of therisk communication comfort zone. PLoS Curr. 2017;9:1-11.
- [Google Scholar]
- Domains of self-uncertainty and their relationship to group identification. J Theor Soc Psychol. 2018;2:67-75.
- [Google Scholar]
- Uncertainty-identity theory. In: Van Lange PA, Kruglanski AW, Higgins TE, eds. Handbook of Theories of Social Psychology. Vol Vol. 2. Thousand Oaks, CA: SAGE; 2012. p. :62-80.
- [Google Scholar]
- Propaganda in an insecure, unstructured world:How psychological uncertainty and authoritarian attitudes shape the evaluation of right-wing extremist internet propaganda. J Deradicalization. 2017;10:203-29.
- [Google Scholar]
- Belief in conspiracy theories:Basic principles of an emerging research domain. Eur J Soc Psychol. 2018;48:897-908.
- [Google Scholar]
- Belief in conspiracy theories:Looking beyond gullibility. In: Forgas JP, Baumeister RF, eds. The Social Psychology of Gullibility. New York: Routledge; 2019. p. :61-75.
- [Google Scholar]
- Conspiracy theories as part of history:The role of societal crisis situations. Mem Stud. 2017;10:323-33.
- [Google Scholar]
- Who do you believe?Political parties and conspiracy theories in Pakistan. Party Politics. 2020;26:107-19.
- [Google Scholar]
- The psychological roots of anti-vaccination attitudes:A 24-nation investigation. Health Psychol. 2018;37:307-15.
- [Google Scholar]
- The role of conspiracist ideation and worldviews in predicting rejection of science. PLoS One. 2013;8:e75637.
- [Google Scholar]
- Unanswered questions:A preliminary investigation of personality and individual difference predictors of 9/11 conspiracist beliefs. Appl Cogn Psychol. 2010;24:749-61.
- [Google Scholar]
- Speaking (un-) truth to power:Conspiracy mentality as a generalised political attitude. Eur J Pers. 2014;28:25-43.
- [Google Scholar]
- National Emergency Action Plan for Polio Eradication. 2015. Global Polio Eradication Initiative. Available from: https://polioeradication.org/wp-content/uploads/2016/07/5.2_14IMB.pdf
- [Google Scholar]
- Hurdles to the global antipolio campaign in Pakistan:An outline of the current status and future prospects to achieve a polio free world. J Epidemiol Community Health. 2013;67:696-702.
- [Google Scholar]
- Refusal of oral polio vaccine in northwestern Pakistan:A qualitative and quantitative study. Vaccine. 2014;32:1382-7.
- [Google Scholar]
- Developing a three-dimensional narrative to counter polio vaccine refusal in Charsadda. J Glob Health. 2020;10:021301.
- [Google Scholar]
- Parental perceptions surrounding polio and self-reported non-participation in polio supplementary immunization activities in Karachi, Pakistan:a mixed methods study. Bull World Health Organ. 2012;90:822-30.
- [Google Scholar]
- Pakistan's expanded programme on immunization:An overview in the context of polio eradication and strategies for improving coverage. Vaccine. 2013;31:3313-9.
- [Google Scholar]
- Challenges to health workers and their opinions about parents'refusal of oral polio vaccination in the Khyber Pakhtoon Khawa (KPK) province, Pakistan. Vaccine. 2016;34:2074-81.
- [Google Scholar]
- English Language in Pakistan's Higher Education. 2015. British Council. Available from: ttps://www.britishcouncil.pk/sites/default/files/english_language_in_pakistan_higher_education_-_2015pdf
- [Google Scholar]
- Psychometric Theory (2 nd ed). United States: McGraw-Hill; 1978.
- Psychometric Theory. New York: McGraw-Hill; 1994.
- PsyToolkit:A software package for programming psychological experiments using Linux. Behav Res Methods. 2010;42:1096-104.
- [Google Scholar]
- PsyToolkit:A novel web-based method for running online questionnaires and reaction-time experiments. Behav Res Methods. 2017;44:24-31.
- [Google Scholar]
- Fearing the uncertain:Self-uncertainty plays a role in mortality salience. J Exp Soc Psychol. 2015;57:31-42.
- [Google Scholar]
- Measuring individual differences in generic beliefs in conspiracy theories across cultures:Conspiracy mentality questionnaire. Front Psychol. 2013;4:225.
- [Google Scholar]
- Declaration of COVID 19 Pandemic. 2020. Ministry of Federal Education and Professional Training. Available from: https://mofept.gov.pk/siteimage/misc/files/notice%20covid-19-1_73135.pdf
- [Google Scholar]
- Statistical Power Analysis for the Behavioral Sciences (2 nd ed). New York: Academic Press; 2013.
- Multivariate Data Analysis (7 th ed). NJ, USA: Prentice Hall; 2009.
- Structural Equation Modeling with EQS and EQS/Windows:Basic Concepts, Applications, and Programming. United Kingdom: Sage; 1994.
- Alternative ways of assessing model fit. In: Bollen KA, Long JS, eds. Testing Structural Equation Models. London, UK: Sage Publications; 1993. p. :136-54.
- [Google Scholar]
- Methodology in the Social Sciences:Principles and Practice of Structural Equation Modeling. New York, US: Guilford Press; 1998.
- Multivariate Data Analysis (5 th ed). New Jersey, USA: Prentice Hall; 1998.
- The moral case for the routine vaccination of children in developed and developing countries. Health Aff (Millwood). 2011;30:1029-33.
- [Google Scholar]
- Knowledge, attitude and perception of polio (Poliomyelitis) among general public in Pakistan. Value Health. 2015;18:A591.
- [Google Scholar]
- The effect of opinion clustering on disease outbreaks. J R Soc Interface. 2008;5:1505-8.
- [Google Scholar]
- Measles outbreaks in a population with declining vaccine uptake. Science. 2003;301:804.
- [Google Scholar]
- The World Uncertainty Index. Working Paper 19-027, Stanford Institute for Economic Policy Research, Stanford University 2018
- [Google Scholar]
- Global Uncertainty Related to Coronavirus at Record High. 2020. IMF Blog. Available from: https://blogs.imf.org
- [Google Scholar]
- The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS One. 2014;9:e89177.
- [Google Scholar]
- Mass Panic, Propaganda, and Mobs:How an Anti-Polio Drive Came to a Screeching Halt in Pakistan. 2019. Radio Free Europe/Radio Liberty. Available from: https://www.rferl.org/a/mass-panic-propaganda-and-mobs-how-an-anti-polio-drive-came-to-a-screeching-halt-in-pakistan/29907091.html
- [Google Scholar]
- Conspiracist ideation in Britain and Austria:Evidence of a monological belief system and associations between individual psychological differences and real-world and fictitious conspiracy theories. Br J Psychol. 2011;102:443-63.
- [Google Scholar]
- Measuring attitudes toward Hijras in Pakistan:Gender and religiosity in perspective. Pak J Psychol Res. 2015;30:151-87.
- [Google Scholar]
- Reaching the last one percent:Progress and challenges in global polio eradication. Curr Opin Virol. 2012;2:188-98.
- [Google Scholar]
- Country profile:Afghanistan. 2008. Library of Congress. Available from https: //www.loc.gov/rr/frd/cs/profiles/Afghanistan.pdf
- [Google Scholar]
- An examination of the factorial and convergent validity of four measures of conspiracist ideation, with recommendations for researchers. PLoS One. 2017;12:e0172617.
- [Google Scholar]
- Uncertainty, entitativity, and group identification. J Exp Soc Psychol. 2007;43:135-42.
- [Google Scholar]




