
Translate this page into:
Developmental dysplasia of the hip in infants younger than six months: Ultrasonographic assessment in relation with risk factors
Address for correspondence: Dr. Fahad Alshehri, Department of Radiology, College of Medicine, Qassim University, Buraydah, Postal Code 52581, Saudi Arabia. E-mail: F.alshehri@qu.edu.sa
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Qassim Uninversity and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives:
In newborns, developmental dysplasia of the hip (DDH) is an abnormal development of the hip joint but its accurate detection is challenging. This study was designed to determine an accurate detection of DDH and their associated risk factors in infants younger than 6 months using sonographic and clinical examinations.
Methods:
Infants younger than 6 months (n = 404) with their hip instability were recruited. Infants’ hips were examined by ultrasonographic and clinical examinations. Ultrasonographic data were accessed in relation with the risk factors. Omni calculator was used to measure sensitivity, specificity and accuracy.
Results:
Out of 808 hips, 97.3% hips were categorized as Graf I type, 1.4% hips were Graf type IIa, 0.87% were type IIb, and 0.49% were type IIc. The data revealed that 93.9% hips were congruous and 6.1% hips were immature. Importantly, the data showed that risk factors such as mode of delivery, breech presentation, oligohydramnios, family history, and malformations were proportionally associated with positive DDH cases. Interestingly, the sensitivity, specificity, and accuracy of ultrasonography in relation with clinical positivity of DDH infants were 51.83%, 99.43%, and 73.16%, respectively.
Conclusions:
This study proved that ultrasonographic assessments are highly sensitive, specific and accurate for the detection of DDH onset in infants younger than 6 months. In addition, the study investigated a number of risk factors associated with the onset of DDH; therefore, it is extremely important that ultrasonography and clinical examination should be performed by those sonographers and orthopedic surgeons, who will have the knowledge of associated risk factors.
Keywords
Clinical assessment
DDH
hip abnormalities
infants
risk factors
ultrasonography

Introduction
Developmental dysplasia of the hip (DDH) is the most common musculoskeletal disorder of the hip in infants.[1] Anatomically, DDH has now been well considered as a gross joint misalignment from the femoral head to the hip socket.[2] A number of factors have been associated with onset of DDH abnormalities including low birth weight, born breech, bearing mother with high estrogen and of course unfavorable surrounding environment of the delivering mother such as social and emotional conditions of the bearing mother.[1,2] An early diagnosis of DDH is very important for the successful treatment as a number of DDH abnormalities occur due to the delay in the diagnosis of DDH.[3] It has now been well established that the Ortolani/Barlow maneuvers is a most powerful and routinely used approach for the detection of DDH and its associated abnormalities in the infants.[4,5] However, the sensitivity, accuracy, and specificity of the clinical examination may vary from case to case especially in the early childhood stage at which the hip joint is mainly composed of cartilage, where the detection of DDH associated abnormalities has always been challenging.[6,7] Sonographic assessment for hip examination in young infants is a key for handling and treating the cases with DDH. These assessments combine the dynamic examination of the hip movement and also include the examination of direct imaging of cartilaginous tissue around the hip joint which is difficult to visualize on simple radiographs.[8,9] The ultrasonography is highly useful for the assessment of hip joint stability especially under the circumstances where the clinical examinations fail to detect the deformities of the hip joint.[8-10] Sonography in combination with clinical examination is highly useful for the diagnosis of DDH in the early weeks of the newborn’s life to start the treatment right away.[11] The DDH and its associated deformities in an early clinical screening have been considered under the category of a continuum of congenital hip disorders.[1,12] A number of disorders have occurred due the delay in a diagnosis of DDH in infants such as elevated surgical intervention and occurrence of crippling end-stage adolescent degenerative hip joint disorders.[8,13] To prevent the onset of disorders associated with DDH due to the delay in diagnosis of DDH in infants, teenagers or children, a number of radiologists are using a variety of ultrasonic techniques including gold standard ultrasonography of infants hips.[14,15] Besides these, femoral head coverage procedures have also been widely used, which measure an acetabular coverage around the femoral head in percentage and this technique has also found to be useful in the diagnosis of DDH and its associated degenerative abnormalities in infants, teenagers and children.[15,16] This study was hypothesized that an accuracy in diagnosis of DDH in infants younger than 6 months prevented the onset of DDH associated structural abnormalities. To test this hypothesis, sonographic examinations were applied for the detection of DDH and their associated risk factors in infants younger than 6 months.
Methods
Patients’ recruitments
This study was performed on 404 infants of <6 months of age (146 male and 258 female), admitted in the Pediatric Department and referred to the Radiology Unit at the Qassim National Hospital, Qassim Saudi Arabia. The protocols of study also conform with The Code of Ethics of the World Medical Association (Declaration of Helsinki), printed in the British Medical Journal. Ethical approval of the study was taken from the Ethical Review Board Committee of the General Directorate of Health Affairs, Al-Qassim Region, Ministry of Health, Saudi Arabia (Ethical Approval Number: 607/44/10435; Dated: July 08, 1444)). Infants of age in mean (±SD) was 15.23 (±4.21) weeks. Informed consents were taken from the infants’ parents
Clinical examination of DDH in early phase
An early clinical examination of DDH on the infants was performed as described by Barlow and Ortolani.[17] Briefly, this examination was based on the clunk, which has been defined as a lost connection between a high pitched and acetabular pathology across neolimbus. The clunk felt is typically known as an “Ortolani sign,” which basically defines the hip lowers into the acetabulum whereas the hip was in abduction.
Clinical examination of DDH in late phase
This type of clinical examination of DDH on the infants was performed in accordance with the Galeazzi sign as described previously.[18] Briefly, the unilateral dislocation of the hip in infants was diagnosed using the Galeazzi sign. This typically determined the hip dislocation on the basis of observation of the displacement in a permanent posture.
Detection of DDH by hip ultrasonographic examination
The DDH in the infants was examined by ultrasonography using a 7 MHz linear array transducer as described previously.[19,20] Experienced sonographers performed ultrasonographic examinations and the findings were analyzed in accordance to the Graf classification as described previously.[21]
Calculation of sensitivity, specificity, accuracy, positive likelihood ratio, and negative likelihood ratio of ultrasonography in relation with clinical positive DDH infants.
The sensitivity, specificity, accuracy, positive likelihood ratio, and negative likelihood ratio between ultrasonography and clinical assessment were directly calculated using an online OMNI calculator.[22]
Statistical analysis
The data used in this study were analyzed by Microsoft Excel program and the results were further validated by Prism GraphPad Ver. 5 software (GSL Biotech, USA). The data were presented in percentage or mean ± SD unless stated otherwise. P < 0.05 considered statically significant.
Results
Ultrasonographic examinations and hip type distribution
A total of 404 infants of <6 months of age who underwent in clinical examination, out of them 146 (36.1%) were male and 258 (63.9%) were female with mean (±SD) age of 15.23 (±4.21) weeks were included in this study. The ultrasonographic examinations of 808 hips of infants with expected DDH and their associated deformities showed various types of hip distributions which are summarized in Figures 1-3. In Figure 1a, we presented distribution of 808 hips evaluation in accordance of Graf classification as follows: Graf type 1 (normal hip) 97.3% (n = 786), Graf type IIa (physiologic immaturity) 1.4% (n = 11), Graf type IIb (acetabular dysplasia) 0.87% (n = 7), and Graft type IIc (critical zone) 0.49% (n = 4). Specifically, right (Rt) hip and left (Lt) hip the Graf types evaluation have been shown in Figure 1b, Graf type 1 Rt hip 97% (n = 392), Graf type IIa Rt 1.5% (n = 6), Graf type IIb Rt 1.0% (n = 4), Graf type IIc Rt 0.5% (n = 2), Graf type 1 Lt 97.5% (n = 394), Graf type IIa Lt 1.2% (n = 5), Graft type IIb Lt 0.74% (n = 3), and Graft type IIc Lt 0.5% (n = 2).
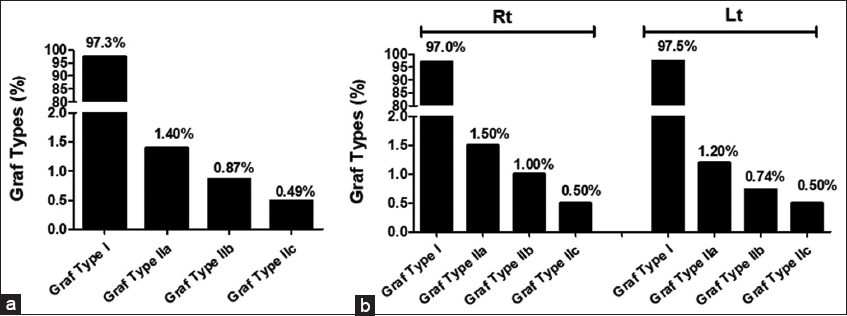
- (a) Ultrasonographic examinations of hip type distribution of 808 hips of affected infants (n = 404) in accordance of Graf classification. Graf type 1 or normal hip (n = 786), Graf type IIa or physiologic immaturity (n = 11), Graf type IIb or acetabular dysplasia (n = 7), and Graft type IIc or critical zone (n = 4). (b) Ultrasonographic examinations of hip type distribution of 404 Right (Rt) hips and 404 Left (Lt) hips of affected infants (n = 404) in accordance of Graf classification. Graf type 1 Rt hip (n = 392), Graf type IIa Rt (n = 6), Graf type IIb Rt (n = 4), Graf type IIc Rt (n = 2), Graf type 1 Lt (n = 394), Graf type IIa Lt (n = 5), Graft type IIb Lt (n = 3), and Graft type IIc Lt (n = 2)
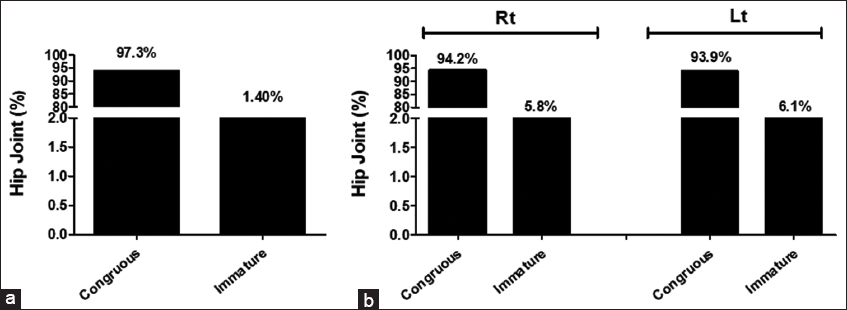
- (a) Ultrasonographic examinations of 808 hip joint distribution of affected infants (n = 404). (b) Ultrasonographic examinations of 404 Right (Rt) hips joint and 404 Left (Lt) hips joint of affected infants (n = 404)
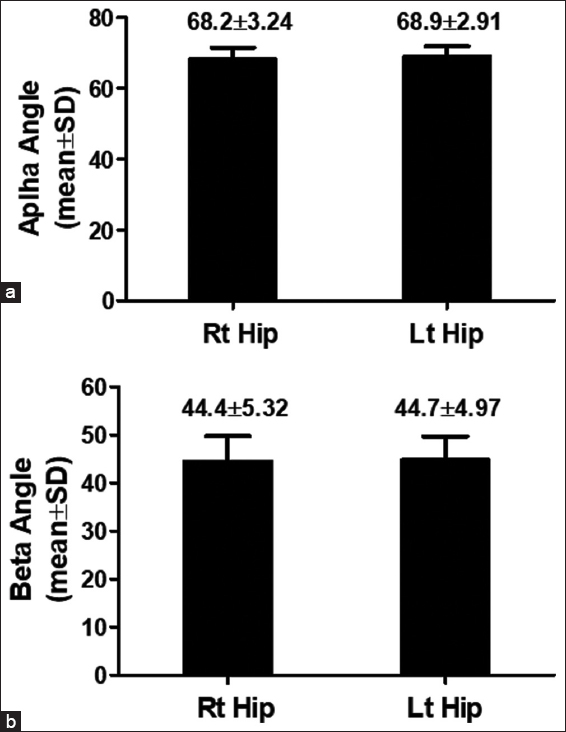
- Ultrasonographic examinations of distribution of Alpha (a) and Beta Angles (b) in 404 Right (Rt) hips joint and 404 Left (Lt) hips joint of affected infants (n = 404).
Ultrasonographic examinations and distribution of hip joint
We evaluated the deformities in hip joints of studied infants and the data have been summarized in Figure 2. Figure 2a summarizes the analysis of total 808 hips and the data revealed that the 759 hips (93.9%) were congruous and 49 hips (6.1%) were immature. To analysis the results in more details, Rt and Lt hips were analyzed separately and the data revealed that the congruous was examined in 94.2% (n = 380) infant’s right (Rt) hip joint, and immature was examined in 5.5% (n = 24) infants Rt hip joint. Whereas in the left (Lt) hip joint, 93.9% (n = 379) infants examined congruously and 6.1% (n = 25) infants Lt hip joint were immature [Figure 2b].
Ultrasonographic examinations of distribution of alpha and beta angles
The Graf method of ultrasound classification system for DDH in infants, describes both alpha and beta angles. In general, the alpha angle has been applied for the determination of the type, whereas the subtype can be determined by beta angles. In this study the mean (±SD) of alpha angle in the studied infants was found to be 68.2 (±3.24) in Rt hips and 68.9 (±2.91) in Lt hips [Figure 3a], whereas the mean (±SD) of beta angle was 44.4 (±5.32) in Rt hips and 44.7 (±4.97) in Lt hips [Figure 3b]. We also presented ultrasound images of infants that showed right alpha and beta angles with bony coverage of type 1 [Figure 4a and b], and ultrasound images that showed right alpha and beta angles with bony coverage of type II b [Figure 4c and d].
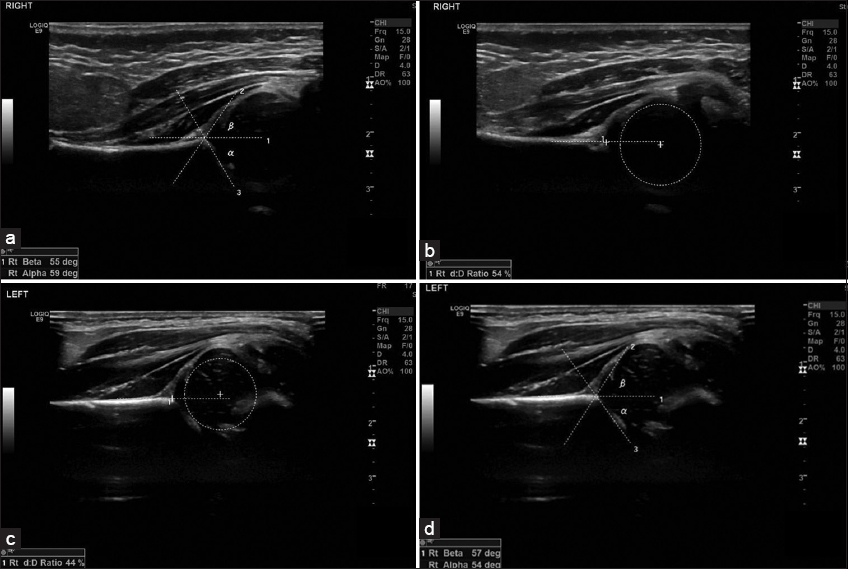
- (a and b) Ultrasound images of right alpha and beta angles with bony coverage of Type 1. (c and d) Ultrasound images of right alpha and beta angles with bony coverage of Type IIb.
Clinical and sonographic assessment of affected infants
Clinical assessment of infants showed that 92.6% (n = 374) patients were having normal hips, they were considered as normal. Whereas unstable hips were found in 6.9% (n = 28) patients; however, irreducible hips joint dislocation were found in 0.5% (n = 2) patients [Figure 5a]. The overall clinical assessment of all 404 patients showed that 7.4% (n = 30) were positive and the rest 92.6% (n = 374) patients were normal [Figure 5b]. Sonographic assessment of all studied infants, showed almost similar results as we obtained with clinical assessment. Out of 404 infants, 88.9% (n = 359) were normal and the rest 11.1% (n = 45) were positive due to the onset of DDH and its associated abnormalities [Figure 5c].
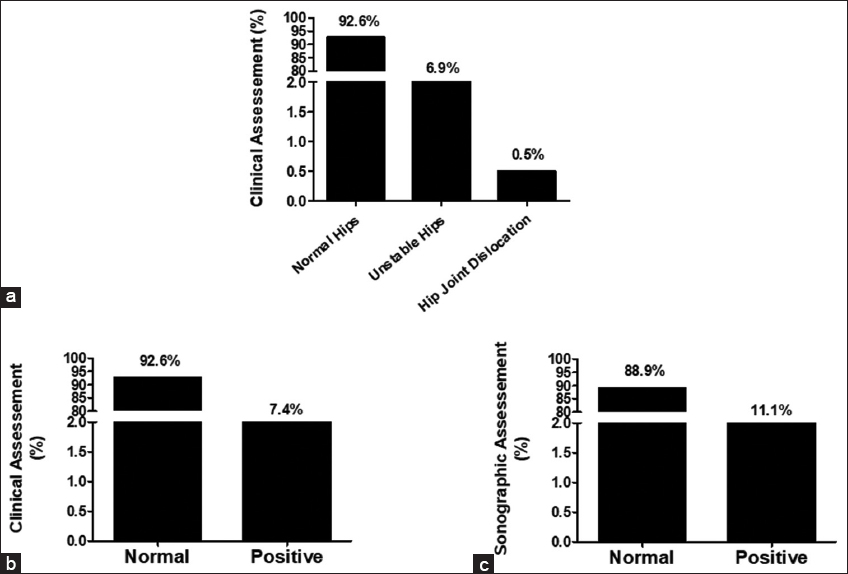
- (a) Clinical assessment of affected infants’ hips. (b) Final outcome of clinical assessment of patients’ hips. (c) Final outcome of sonographic assessment of patients’ hips
Risk factor associated with DDH onset
We determined the possible risk associated with affected infants and mode of delivery of infants has been considered to be also a factor associated with risk of DDH onset. First, we studied a thorough background of the affected infants and determined that mode of delivery, breech presentation, oligohydramnios, family history, and malformations, these factors were significantly associated with the prevalence of DDH. Out of 404 studied infants, 138 (34.2%) infants were delivered through caesarean delivery (CD), whereas the rest 266 (65.8%) were delivered through natural vaginal delivery (NVD) [Figure 6a]. The risk factors other than mode of delivery were also studied such as breech presentation, oligohydramnios, family history and associated malformations. The data showed that breech presentation, oligohydramnios, family history and associated malformations were found in 100 (24.7%) infants, 14 (3.5%) infants, 23 (5.7%) infants, and 20 (4.95%) infants, respectively [Figure 6b].
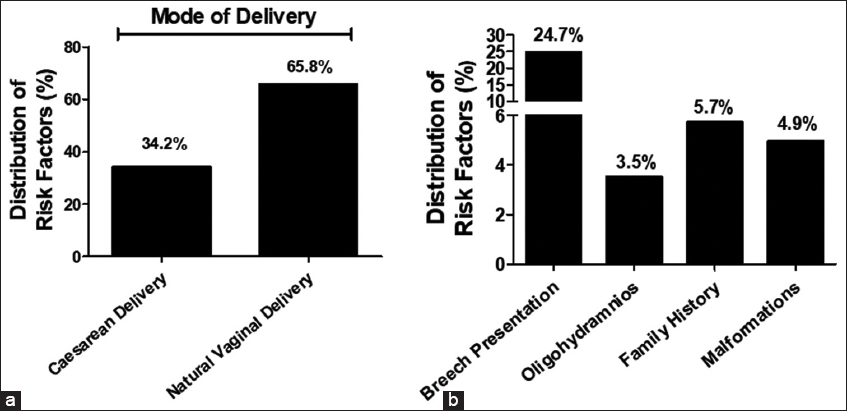
- Distribution of risk factor associated with DDH onset (a) Mode of delivery - caesarean delivery (n = 138) and natural vaginal delivery (n = 266) (b) Breech presentation (n = 100), oligohydramnios (n = 14), family history (n = 23), and associated malformations (n = 20).
Ultrasonographic assessment in relation with risk factors associated with DDH onset
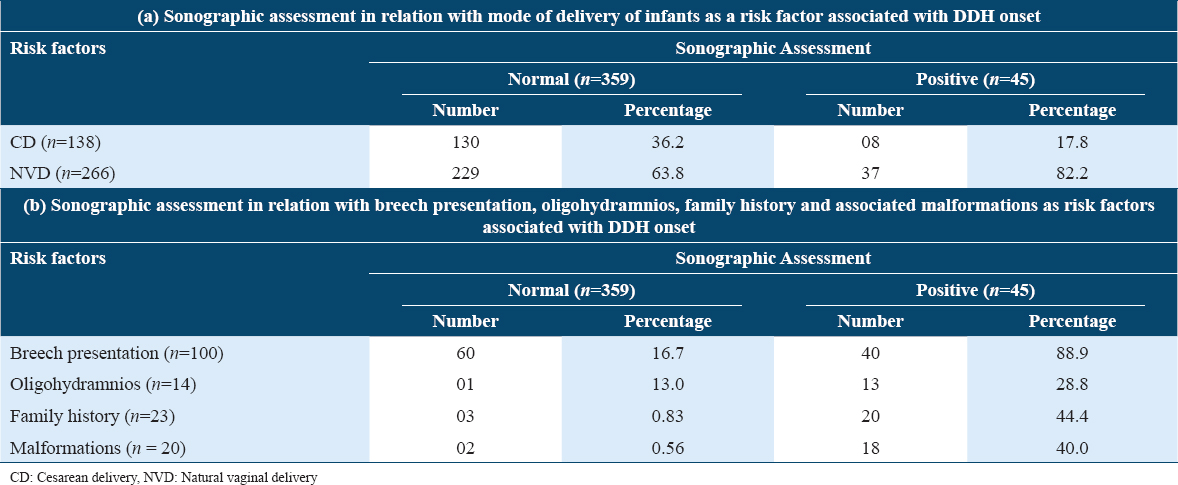
We also studied the sonographic assessment in relation to the risk factors. The sonographic findings showed that mode of delivery-CD was found to be normal in 36.2% infants and 17.8% infants were found to be positive. Whereas, mode of delivery-NVD was normal in 63.8% infants and 82.2% infants were positive [Figure 7a]. Breech presentation was found to be normal in 16.7% cases, whereas it was to be positive in 88.9% [Figure 7b]. The risk factor oligohydramnios was found to be normal in 0.3% cases, whereas it was positive in 28.8% cases [Figure 7c]. The other risk factor family history was found to be normal in 0.83% infants, whereas it was positive in 44.4% infants [Figure 7d]. On the other hand, associated malformations risk factor was normal in 0.5% infants, whereas it was positively associated in 40.0% cases [Figure 7e]. All together the ultrasonographic assessment in relation with all DDH associated risk factors is summarized in Table 1.
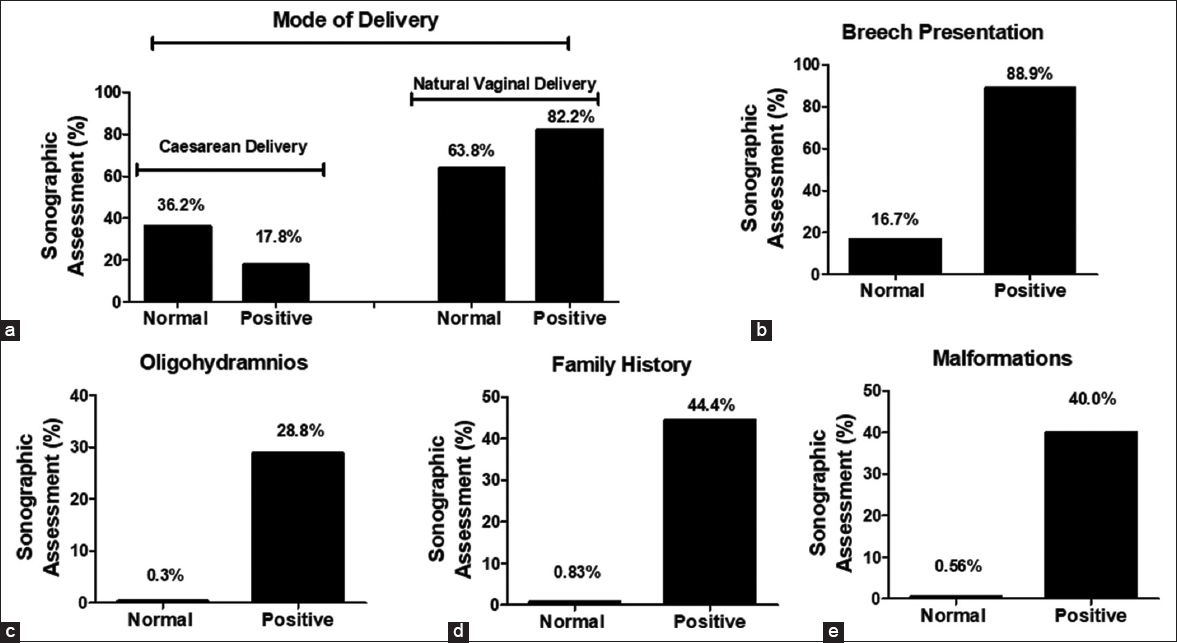
- Sonographic assessment in relation with risk factor associated with DDH onset. Sonographic assessment in relation with mode of delivery - cesarean delivery (n = 138) and natural vaginal delivery (n = 266) (a), breech presentation (n = 100) (b), oligohydramnios (n = 14) (c), family history (n = 23) (d), and associated malformations (n = 20) (e)
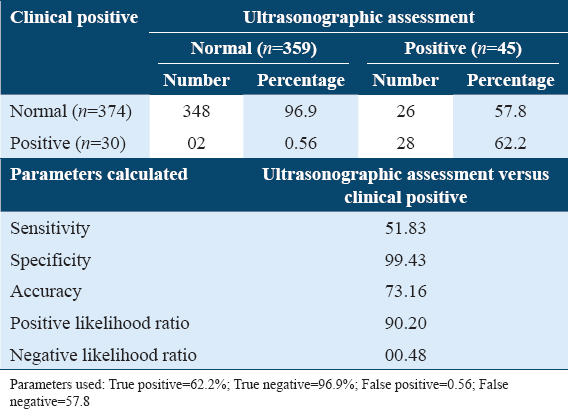
Quantification of sensitivity, specificity, accuracy, positive likelihood ratio, and negative likelihood ratio of ultrasonography in relation with clinical positive of DDH infants.
Using the OMNI calculator, the sensitivity, specificity, accuracy, positive likelihood ratio, and negative likelihood ratio of ultrasonography in relation with clinical positivity of DDH infants were calculated to be 51.83%, 99.43%, 73.16%, 90.2, and 0.48, respectively. The complete details of clinical positive and sonographic assessment are summarized in Table 2.
Discussion
This study proved that ultrasonography assessment is highly useful for the detection of the DDH and their associated risk factors in infants younger than 6 months. Diagnosis of DDH and their associated deformities has always been a challenge in newborn or in infants younger than 6 months.[23,24] The clinical examination of the infant’s hip is not always enough in detecting DDH alone, as there will always be chances of some dysplasia, un-stability of hip joint, dislocation, or subluxated hips especially when examined by inexperienced clinical examiners, they may have falsely considered a normal hip as pathogenic. Several studies documented that ultrasonography is a very useful, precise, non-invasive technique for the diagnosis of DDH and their associated structural abnormalities but still complications have been associated when the technique applied for newborn and infants younger than 6 months. Therefore, experienced sonographers and experienced clinical examiners are extremely necessary.[25,26] To avoid the reporting of false positive diagnosis of DDH and their associated deformities in infants younger than 6 months, this study was designed to determine the best possible ways for identification of DDH. A total of 404 infants of <6 months of age were recruited in this study, who underwent a clinical examination for hips problems. The clinical examination of the infant’s hips in this study was performed in accordance with Barlow and Ortolani techniques.[17] Clinical assessment of infants in this study showed that 92.6% patients were having normal hips, they were considered as normal. Whereas unstable hips were found in 6.9% infants; however, irreducible hips joint dislocation were found in 0.5% cases. The overall clinical assessment of all 404 patients showed that 7.4% were clinically positive and the rest 92.6% were clinically normal.
Studies have shown that imaging techniques such as ultrasonographic screening have detected cartilage, aberrant alignment of the femoral head within the acetabulum, instability, and dysplasia.[25,26] In accordance with these, this study performed ultrasonographic examinations of 808 hips of infants with expected DDH and their associated deformities and showed various types of hip distributions. Out of 808 hips, the Graf type 1 (normal hip) was analyzed in 786 hips, whereas Graf type IIa (physiologic immaturity) were detected in 11 hips, Graf type IIb (acetabular dysplasia) was analyzed in 7 hips, and Graft type IIc (critical zone) was detected in 4 hips. These ultrasonographic findings determined how the femoral head in relation with acetabulum varies in different stages of DDH in different Graf’s types.[21,27] In this study, we evaluated the deformities assessment in 808 hips and the data revealed that the 759 hips were congruous and 49 hips were immature in infants younger than 6 months. To analyze the results in depth, Rt and Lt hips were analyzed separately and the data showed that the congruous was examined in 380 infants right (Rt) hip joint, and immature was examined in 24 infants Rt hip joint. Whereas in the left (Lt) hip joint, 379 infants hips examined as congruous and 25 infants Lt hip joint were immature. Concerning about Graf types in Rt and Lt hips of studied subjects, Rt hip and Lt hip the Graf types evaluation. The Graf type 1 was found in 392 Rt hips, Graf type IIa was in 6 Rt hips, Graf type IIb was found in 4 Rt hips and Graf type IIc was found in 2 Rt hips of the studied infants. Whereas the Graf type 1 was found in 394 Lt hips, Graf type IIa was found in 5 Lt hips, Graft type IIb 3 Lt hips and Graft type IIc was in 2 Lt hips of the infants. These findings clearly indicated that both Rt and Lt hips were equally impacted due DDH. These results have also been fully supported by other studies.[28-31] In contrast to these published reports and the findings described in this study, few studies also point out that Lt hips were most commonly impacted due to DDH as compared with the Rt hips[25,32] and the reason they expected that fetal position of Lt occiput anterior causes adduction of the Lt hip which is in proximity to the maternal sacrum,[25,32] but the available evidence to prove and to support this statement are not enough.
In this study, we investigated the possible risk associated with the prevalence of DDH in infants younger than 6 months. First, we studied a thorough background of the affected infants and determined that mode of delivery, breech presentation, oligohydramnios, family history, and malformations, these factors were significantly associated with the prevalence of DDH. Then, we also studied these risk factors via sonographic assessment. The sonographic findings showed that cesarean delivery was found to be positively associated in 17.8% infants, whereas, NVD was positively associated in 82.2% infants. Breech presentation, oligohydramnios, family history and malformations were positively associated with the onset of DDH in 88.9%, 28.8%, 44.4%, and 40.0% of studied infants. These positive associations of risk factors with DDH prevalence have also been supported by a number of studies,[33-37] but the pattern of association of risk factors with the prevalence of DDH that we discovered has never been discovered previously. Finally, the study also determined the ultrasonographic sensitivity, specificity, and accuracy in relation with the clinical assessments and findings showed that the ultrasonographic measurements were highly sensitive, specific, and accurate.
Conclusion
This study proved that ultrasonographic assessments are highly sensitive, specific and accurate for the detection of DDH onset in infants younger than 6 months. In addition, the study investigated a number of risk factors associated with the onset of DDH such as mode of delivery of infants, breech presentation, oligohydramnios, family history, and malformations. Therefore, it is highly recommended that ultrasonography and clinical examination should be performed by those sonographers and orthopedic surgeons, who will have complete knowledge of risk factors associated with the prevalence of DDH and their associated deformities in infants younger than 6 months.
Authors Declaration
Ethics approval and consent to participate
Ethical approval of this study was taken from the Ethical Review Board Committee of the General Directorate of Health Affairs, Al-Qassim Region, Ministry of Health, Saudi Arabia (Ethical Approval Number: 607/44/10435; Dated: July 08, 1444). The protocols of study also conform with The Code of Ethics of the World Medical Association (Declaration of Helsinki), printed in the British Medical Journal. Informed consents were taken from the infants’ parents.
Availability of data and materials
The data sets used in this study are available with corresponding author and will be provided on a reasonable request.
Competing interest
The authors have no conflict of interest to declare.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author’s contribution
FA performed conceptualization, design, data analysis, and manuscript drafting. YA performed data collection and manuscript revision. Both authors have critically reviewed and approved the final draft and are responsible for the content of the manuscript.
Acknowledgment
The authors gratefully acknowledged to all participants’ parents’ and the generous support of the Qassim National Hospital in completing this important project.
References
- Progress in screening strategies for neonatal developmental dysplasia of the hip. Front Surg. 2022;9:995949.
- [Google Scholar]
- Incidence of neonatal developmental dysplasia of the hip and late detection rates based on screening strategy:A systematic review and meta-analysis. JAMA Netw Open. 2022;5:e2227638.
- [Google Scholar]
- Effectiveness of different types of ultrasonography screening for developmental dysplasia of the hip:A meta-analysis. Medicine (Baltimore). 2020;99:e23562.
- [Google Scholar]
- A reappraisal of the Ortolani examination in children with developmental dysplasia of the hip. J Pediatr Orthop. 2007;27:27-31.
- [Google Scholar]
- Factors for selective ultrasound screening in newborns with developmental dysplasia of the hip (DDH) . Front Surg. 2022;9:1038066.
- [Google Scholar]
- Comparing results of clinical versus ultrasonographic examination in developmental dysplasia of hip. J Res Med Sci. 2013;18:1051-5.
- [Google Scholar]
- Early detection of developmental dysplasia of hip by ultrasound. Hip Int. 2021;31:424-9.
- [Google Scholar]
- Developmental dysplasia of the hip:A review. J Long Term Eff Med Implants. 2022;32:39-56.
- [Google Scholar]
- Developmental dysplasia of the hip in infants referred for a combined pediatric orthopedic and radiologic examination. A prospective cohort study. J Orthop. 2022;32:109-14.
- [Google Scholar]
- Developmental dysplasia of the hip:An audit of the ultrasound screening programme. Ir Med J. 2022;115:598.
- [Google Scholar]
- Diagnostic performance of clinical examination versus ultrasonography in the detection of developmental dysplasia of hip:A systematic review and meta-analysis. Arch Bone Jt Surg. 2022;10:403-12.
- [Google Scholar]
- The effect of the design of the orthosis on the axial load transmission of two flexion abduction orthoses used in treating congenital hip dysplasia. Heliyon. 2022;8:e11942.
- [Google Scholar]
- Cochrane review:Screening programmes for developmental dysplasia of the hip in newborn infants. Evid Based Child Health. 2013;8:11-54.
- [Google Scholar]
- Correlation between ultrasonic and radiographic imaging of developmental dysplasia of the hip. J Child Orthop. 2019;13:155-60.
- [Google Scholar]
- Developmental retardation of femoral head size and femoral head ossification in mild and severe developmental dysplasia of the hip in infants:A preliminary cross-sectional study based on ultrasound images. Quant Imaging Med Surg. 2023;13:185-95.
- [Google Scholar]
- Which acetabular landmarks are the most useful for measuring the acetabular index and center-edge angle in developmental dysplasia of the hip?A comparison of two methods. Clin Orthop Relat Res. 2020;478:2120-31.
- [Google Scholar]
- Hip Dislocation. Available from: https://www.nabilebraheim.blogspot.com/2017/11/barlow-ortolani-signsddh-congenital-hip.html
- The reliability of ultrasonography in developmental dysplasia of the hip:How reliable is it in different hands? Indian J Orthop. 2015;49:610-4.
- [Google Scholar]
- Using the graf method of ultrasound examination to classify hip dysplasia in neonates. Autops Case Rep. 2012;2:5-10.
- [Google Scholar]
- ONMI Calculator. Available from: https://www.omnicalculator.com/statistics/sensitivity-and-specificity
- Screening of newborns and infants for developmental dysplasia of the hip:A systematic review. Indian J Orthop. 2021;55:1388-401.
- [Google Scholar]
- Screening programmes for developmental dysplasia of the hip in newborn infants. Cochrane Database Syst Rev. 2011;2011:CD004595.
- [Google Scholar]
- Use of ultrasonography in developmental dysplasia of the hip. J Child Orthop. 2014;8:105-13.
- [Google Scholar]
- Ultrasound in the diagnosis of developmental dysplasia of the hip in newborns The European approach. A review of methods, accuracy and clinical validity. Eur Radiol. 2007;17:1960-7.
- [Google Scholar]
- Morphological development of the hip in normal infants under six months of age by the graf ultrasound method. Front Pediatr. 2022;10:914545.
- [Google Scholar]
- 2006. Screening for Developmental Dysplasia of the Hip [Internet]. Rockville MD: Agency for Healthcare Research and Quality (US); Available from: https://www.ncbi.nlm.nih.gov/books/NBK33422
- Screening for developmental dysplasia of the hip:A systematic literature review for the US preventive services task force. Pediatrics. 2006;117:e557-76.
- [Google Scholar]
- Clinical and sonographic improvement of developmental dysplasia of the hip:Analysis of 948 patients. J Orthop Surg Res. 2022;17:538.
- [Google Scholar]
- Effectiveness of ultrasound screening for developmental dysplasia of the hip. Arch Dis Child Fetal Neonatal Ed. 2005;90:F25-30.
- [Google Scholar]
- Development dysplasia of the hip from birth to six months. J Am Acad Orthop Surg. 2000;8:232-42.
- [Google Scholar]
- Associations between risk factors and developmental dysplasia of the hip and ultrasonographic hip type:A retrospective case control study. J Child Orthop. 2019;13:161-6.
- [Google Scholar]
- Borderline developmental dysplasia of the hip:A risk factor predicting the development and poor prognosis after core decompression for idiopathic osteonecrosis of the femoral head. Orthop Surg. 2022;14:2427-35.
- [Google Scholar]
- Is prematurity a risk factor for developmental dysplasia of the hip?A systematic review and meta-analysis. J Pediatr Orthop B 2022 Doi:10.1097/BPB.0000000000001021
- [Google Scholar]
- Developmental dysplasia of the hip and associated risk factors in Saudi children:A retrospective study. J Back Musculoskelet Rehabil. 2021;34:573-80.
- [Google Scholar]
- Risk factors for developmental dysplasia of the hip:A meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2012;165:8-17.
- [Google Scholar]




