
Translate this page into:
The relationship between phytoestrogen-rich supplements and breast cancer: A multicenter case–control study in Saudi Arabia
Address for correspondence: Sahar M. Alnefaie, Department of Surgery, Taif University, Taif, Saudi Arabia. Phone: (+966)557010088. E-mail: sahar.m@tu.edu.sa
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Qassim Uninversity and was migrated to Scientific Scholar after the change of Publisher.
Abstract
ABSTRACT
Objectives:
The prospective effect of phytoestrogen-rich supplements has been explored by many researchers in an attempt to reduce breast cancer (BC) risk worldwide. In Saudi Arabia, some widely used supplements have high phytoestrogen content. Therefore, we aimed to (1) assess the relationship between phytoestrogen supplements (PSs) that are widely used among women of Saudi Arabia and BC and (2) assess the relationship based on the menstrual status.
Methods:
The study took place during 2020–2022 to assess several PSs using a case–control design that included five centers from different provinces around the country. A questionnaire was answered by the participants that included 381 (46%) cases (diagnosed with BC) and 449 (54%) controls (free of BC). The PS items were assessed individually and on the multivariant analysis model.
Results:
Of the 12 phytoestrogen-rich supplements, soy milk showed a significant decrease in BC risk. However, Echinacea showed an increased risk of BC among its users. A subgroup analysis based on the menstrual status demonstrated an increased risk of BC among licorice root and green tea users on premenopausal and postmenopausal women, respectively.
Conclusion:
Soy isoflavones continue to show a significant risk reduction that could be used for a modified approach to reduce the risk of BC. However, Echinacea, licorice root, and green tea have shown to increase the risk of BC.
Keywords
Breast cancer
Echinacea
green tea
licorice root
soy isoflavones

Introduction
Globally, breast cancer (BC) is the most commonly diagnosed cancer among women and the leading cause of death among female cancer patients.[1] Even on a local scale, BC is the most commonly diagnosed cancer in Saudi Arabia, where it accounts for 16.7% of all cancers among Saudis and 30.1% of all cancers among Saudi women.[2] Arab women tend to have BC earlier than Western women by at least a decade.[3]
During the 1920s, the first studies examined the estrogenic activity of plant extracts.[4] This type of exogenous estrogen is known as phytoestrogen.[4] Phytoestrogens comprise two groups: Flavonoids (which include isoflavones, coumestans, and prenylflavonoids) and non-flavonoids (mainly lignan).[4] A total of 70–80% of BCs have the estrogen receptor α (ERα), which is associated with positive or hormone-sensitive cancers.[4]
As a result of structural similarities between phytoestrogen and 17 β-estradiol, there is controversy regarding the uses of phytoestrogen supplements (PSs) and the risk of BC.[5] Phytoestrogen might have estrogenic or anti-estrogenic effects on BC cells,[5,6] and multiple studies suggest that phytoestrogen could promote their proliferation through an interaction with the estrogenic signaling pathway.[5-7] Moreover, a study in the United Arab Emirates found that the 10 most widely used phytoestrogen-containing plants in the Middle East are significantly associated with an increased risk of BC.[6]
Other studies indicate that phytoestrogen has protective or inhibitory effects against BC cells.[8-10] A recent systemic review, which included 127 articles, investigated the effects of soy isoflavones on BC. The results indicated that soy isoflavones may reduce the risk of BC and the recurrence rates among those who were previously diagnosed with BC.[8] Certain subtypes of BC cells have a higher affinity to ER-β than ER-α; therefore, anti-cancerous or anti-proliferative effects could occur through stimulating ER-β.[9]
Saudi Arabia has the highest scientific-research output among Arab countries.[11] Therefore, the present study aims to assess (1) the relationship between phytoestrogens-containing supplements that are widely used among women of Saudi Arabia and BC and (2) the relationship between phytoestrogens-containing supplements and BC based on the menstrual status.
Methods
Study design and setting
This observational retrospective case–control study assesses the risk of PSs in regard to BC. Five hospitals from different regions in Saudi Arabia participated in the study: (1) Prince Sultan Military Medical City, Riyadh; (2) Alhada Hospital for Armed Forces, Taif; (3) King Fahad Hospital of the University, Alkhobar; (4) King Salman Armed Forces Hospital, Tabuk; and (5) King Abdullah Hospital, Bisha. The institutional review board (IRB) at each of the participating hospitals approved the study. The study took place in 2021 and compared those who were diagnosed with BC to those who had been free of BC in the past 4 years.
Study participants and case/control definition
The participants were divided into case and control groups to measure the amount of exposure per group to each specific PS that each study participant consumed. Cases consisted of women who were diagnosed with BC at breast surgery clinics and oncology departments. The controls comprised those who had not been diagnosed with BC according to general surgery and family medicine clinics.
A non-randomized consecutive approach was used to review the electronic medical records system. Reports were obtained from each of the mentioned areas and included every possible medical record number that matched the eligibility criteria: (1) Women who were Saudi Arabian residents and (2) women over the age of 20. Exclusion criteria included (1) terminally ill patients, (2) expired patients, and (3) those who were lost to follow-up in the clinic for more than 3 years.
Patients were requested to fill out an online questionnaire that was used to gather information from participants through self-administration or personal interviews. Only 830 participants out of 1400 responded and answered the questionnaire (381 [46%] cases and 449 [54%] controls); however, the number of respondents was evenly collected among the participating hospitals.
Data source and measurement
The research team developed a self-administered questionnaire which include two sections to assess the study objectives: (1) A section that assessed the participants’ risk factors from their medical history, reproductive history, and lifestyle factors (seen in Table 1) and (2) a section that assessed the frequency and amount for each PSs.
The questionnaire involved 12 PSs, and all of these PSs were in the form of phytoestrogen-rich natural food supplements, such as flaxseed, lentils, and chamomile, which are shown in Table 2. To evaluate the frequency of supplement use, participants were asked, “How often do you use the following supplements?” They could choose one of the following answers: never, 1 time per month, 2–3 times per month, 1 time per week, 2 times per week, 3–4 times per week, and daily. In addition, the portion size was estimated by asking, “How much of the chosen supplements do you use each time?” They could choose one of the following: Half cup or less and half a cup or more. Demonstrations through different alternative names and images of each supplement were used to ensure participants recognized them correctly and to eliminate bias related to the different supplements’ nomenclatures.
PSs and potential cofounders
The research team reviewed the literature to identify which plants are known for their phytoestrogen content and whether they have been used in Saudi Arabia or not. Several plants were identified and these are described in Table 2.
Many well-known relative risk factors for BC exist, which can be non-modifiable risk factors, such as genetic and family history, or modifiable risk factors, such as smoking. These risk factors were considered as confounders in this study. These factors were described and measured for both cases and controls as baseline characteristics and are described in Table 1.
Statistical analysis
Data were analyzed using IBM SPSS Statistical software for Windows version 26.0 (IBM Corp., Armonk, New York, USA). For descriptive statistics, frequencies and percentages were used to describe the categorical variables. Pearson’s Chi-square test and odds ratios were used to test and measure the association between the categorical study variables and outcome variables, cases (BC), and controls (free of BC). Multivariate binary logistic regression was used to identify the independent risk factors associated with BC. A P ≤ 0.05 and 95% confidence intervals were used to report the statistical significance and precision of results.
Results
Association of sociodemographic and clinical characteristics with BC
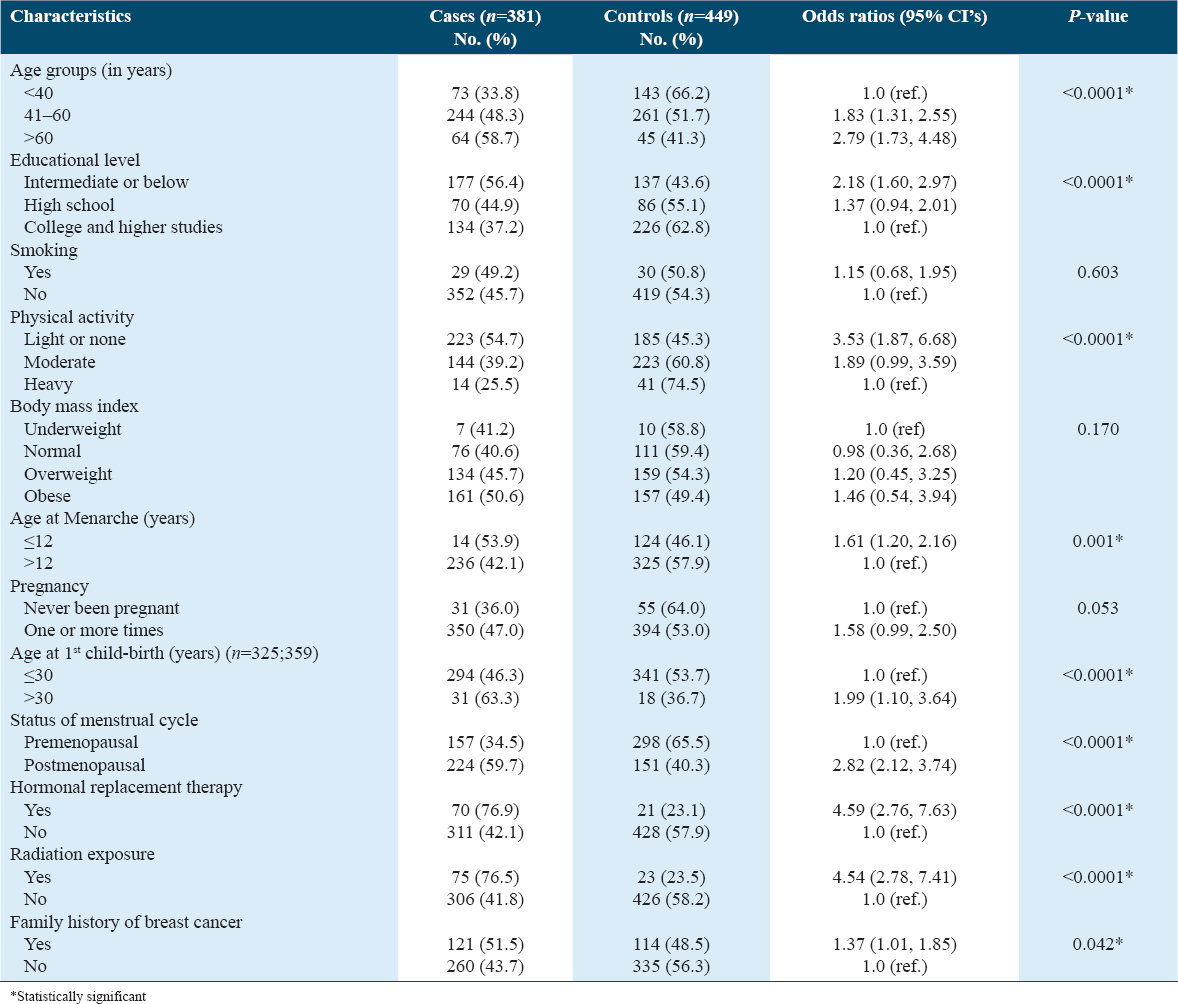
A total of 830 study subjects were used in this analysis, where there were 381 cases (BC) and 449 controls (free of BC). The bivariate analysis for the association between sociodemographic and clinical characteristics and BC shows highly statistically significant associations between age groups, educational level, physical activity, age at menarche (in years), age at first childbirth, status of menstrual cycle, hormonal replacement therapy, radiation exposure, and family history of BC. The odds ratios of two age groups (41–60 and >60 years) indicated that subjects in the age range of these two groups having BC were 1.83 times and 2.79 times higher, respectively, than subjects who were under 40 years of age. The odds ratios of subjects with an intermediate educational level having BC were 2.18 times higher when compared with those who had college and higher education. The other level of education (high school) was not statistically significantly associated with BC.
Regarding the two levels of physical activity (light or none and moderate), the odds ratios indicated that subjects who had light or none and moderate physical activity were 3.52 times and 1.89 times more likely, respectively, to have BC, when compared with subjects who did heavy physical activity. The odds ratio of subjects whose age at menarche was ≤12 years having BC was 1.61 times greater when compared with subjects whose age at menarche was >12 years. Subjects who had their first childbirth >30 years were 1.99 times more likely to have BC compared with those whose age at first childbirth was >30 years.
The odds ratios of subjects with postmenopausal menstrual cycle having BC were 2.82 times greater when compared with subjects who were premenopausal. Subjects who had received hormonal replacement therapy were 4.59 times more likely to have BC compared with subjects who did not receive hormonal replacement therapy. The odd ratios of subjects who exposed to radiation having BC were 4.54 times higher than subjects who had not been exposed to radiation. Finally, the odds of subjects who had a family history of BC having BC were 1.37 times greater than those who did not have a family history of BC. The other characteristics (smoking, BMI, and number of pregnancies) were not statistically significantly associated with BC as shown in Table 1.
Association between items of PS consumption and BC
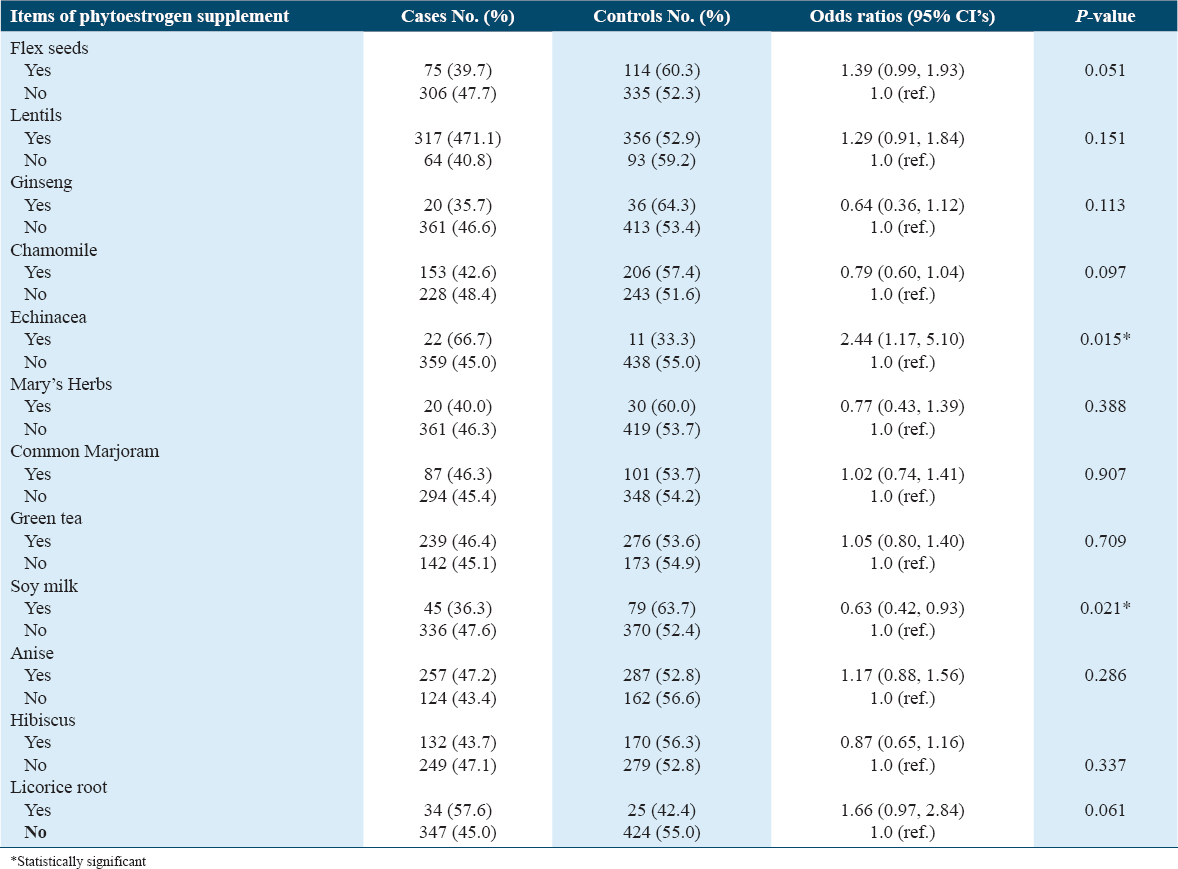
The association of different items of PS consumption and BC shows a statistically significant association between Echinacea and soy milk. The supplement item “Echinacea” is associated with BC as a “risk factor,” where its odds ratio indicated that subjects who consumed Echinacea having BC was 2.44 times higher than those who did not consume the supplement Echinacea, which is statistically significant (P = 0.015). However, the supplement, “soy milk” is associated with BC as a “protective factor,” where its odds of 0.63 show that 37% of subjects who consumed soy milk were protected from BC when compared with those who did not consume soy milk, which is statistically significant (P = 0.021). All other supplement items are not statistically significantly associated with BC, as seen in Table 2.
Association of items of PS consumption with BC in premenopausal and postmenopausal women
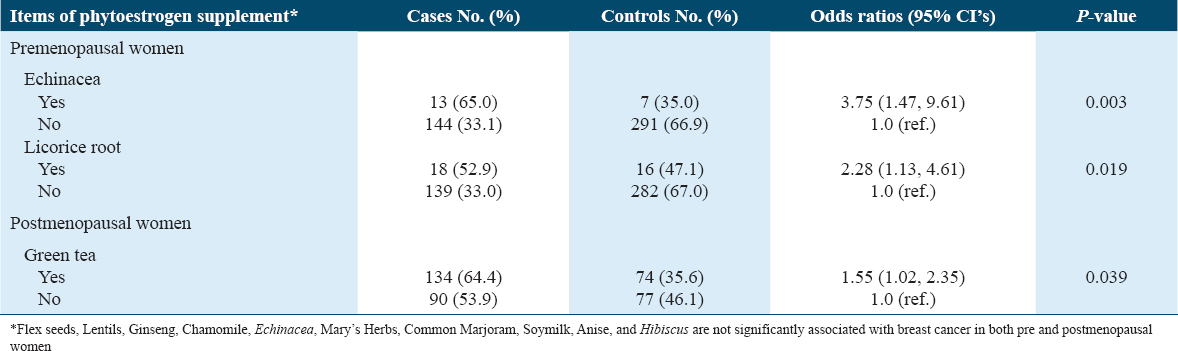
The cases and controls were stratified as per their menstrual cycle (premenopausal and postmenopausal). The bivariate analysis of the association between supplemental items and BC showed a statistically significant association of items (Echinacea and licorice root) with BC in premenopausal women. It also showed a statistically significant association of green tea with BC in postmenopausal women. The corresponding odd ratios of these three items, 3.75, 2.28, and 1.55, indicate that those subjects with premenopausal status who had consumed Echinacea and licorice root were 3.75 times and 2.28 times more likely to have BC than those who did not consume Echinacea and licorice root. In addition, subjects with a postmenopausal status who had consumed green tea were 1.55 times more likely to have BC than those who did not consume green tea, as seen in Table 3.
Multivariate analysis
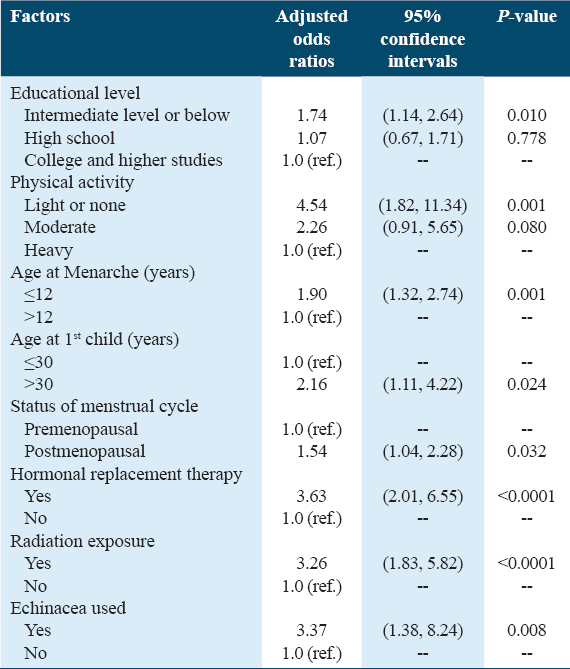
A multivariate binary logistic regression was carried out to identify the independent risk factors associated with BC using the significant variables which were found in bivariate analysis. The model with variables including educational level (intermediate level or below), physical activity (light or none), age at menarche (≤12), age at first childbirth (>30 years), menstrual cycle status (postmenopausal), hormonal replacement therapy (Yes), radiation exposure (Yes), and consumption of Echinacea (Yes) against the models with only constant was statistically significant. This indicates the above variables as a set distinguishing between the subjects who had BC and those who did not (χ2 = 148.701, df = 16, P < 0.0001).
The Hosmer and Leesha test which tests for the goodness of fit for logistic regression models (an alternative to the Chi-square test) had a value of 3.436 (df = 8; P = 0.904). This non-significance indicates that the model prediction does not significantly differ from the observed. Adeleke’s R2 of 0.261 indicates a moderate relationship between prediction and grouping. The final model validation was carried out using a classification table, which summarizes the observed group and the predicted group classification. The overall prediction success was 68.7% (65.2% for case [BC] and 71.9% for control [no BC]). The corresponding adjusted odds ratios indicate a highly independent statistically significant association with BC. The other variables in the model, which are not independently significantly associated with BC, were age groups, family history of BC, use of flax seeds, used of soy milk, and use of licorice root [Table 4].
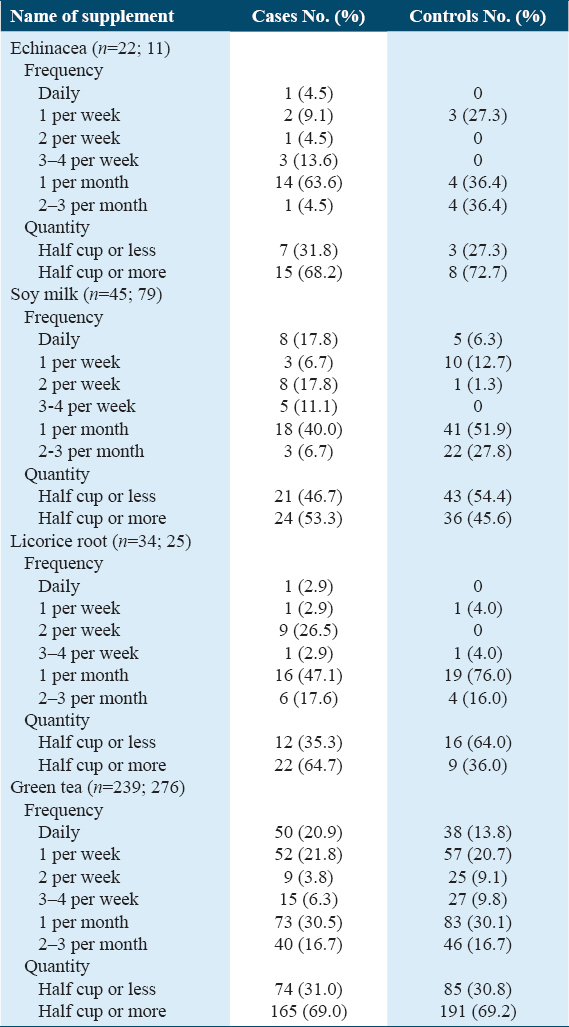
Analysis of significantly associated supplement items frequency and quantity
Table 5 shows the frequency and quantity of four supplement items (Echinacea, soy milk, licorice, and green tea). The frequency of the item Echinacea, which shows as a risk factor for BC in both bivariate and multivariate analysis, shows cases that had consumed Echinacea more frequently (13.6% at 3–4 per week, 63.6% at 1 per month) compared with controls (0% at 3–4 per week and 36.4% at 1 per month). Whereas the frequency use of soy milk, which shows as protective factor for BC in bivariate analysis, shows that controls consumed the product more frequently than cases. In addition, licorice and green tea, which were shown as risk factors for BC in bivariate analysis, indicate that cases consumed the products more frequently than controls.
Discussion
Phytoestrogens have many endocrine and metabolic effects similar to endogenous estrogen.[4] They are molecules with a plant origin and are found in our daily diet, especially in vegetables, legumes, and cereals.[4] The current study is the first study in the Kingdom of Saudi Arabia to assess the influence of phytoestrogen-rich supplements that are commonly used among Saudi women on BC risk. We found that few individuals using phytoestrogen-rich supplements are associated with a significant increase in BC risk. Our results demonstrated that Echinacea was associated with a significant increase in the risk of BC. When the risk was stratified based on menstrual status, licorice and green tea were associated with a significant increase in BC risk in premenopausal and postmenopausal women, respectively. However, soy milk was the only phytoestrogen-rich supplement that significantly decreased the risk for BC.
Echinacea is one of the most popularly used herbal supplements among BC patients.[12] Studies have evaluated the potentials of Echinacea extracts as a candidate to reduce the growth of BC cells.[12-14] Tang et al. have investigated the inhibitory effect of the Echinacea small molecule extract known as “Echinacoside” on BC cells. The results showed inhibitory potentials of echinacoside on proliferation, migration, and the signaling pathway of BC cells.[13] A similar conclusion was reached in another report, which showed that extracts of Echinacea purpurea had the potential to reduce the growth of mammalian BC cells.[14] Contrary to the findings of these studies, we found that Echinacea was associated with an increased risk of BC among the women of Saudi Arabia.
Licorice roots and green tea are common beverages among people of the Middle East and worldwide with a wide public belief in their health benefits.[15,16] Licorice root has been investigated for its anti-cancerous extract known as isoliquiritigenin (ISL).[15] This is a subclass of flavonoids that have ERs agonist in both in vivo and in vitro.[17] In fact, several studies have concluded that ISL suppresses the growth of MCF7 BC cells in culture experiments, and it has chemopreventive potential on BC cells; however, it has also been found that it exhibits a biphasic pattern when it influences the MCF7 cell line.[17-19] Maggiolini et al. demonstrated that low concentrations of ISL specifically promoted the proliferation of MCF7 cells, conversely to high concentrations that exhibit a cytotoxic effect. Thus, the long-term exposure to low ISL concentrations could promote the progression of estrogen-dependent BC.[17] It is interesting to note that licorice roots have been shown to increase the risk of BC among premenopausal women in our study. On the other hand, catechins of green tea belong to the flavonoids group, and they are known for their anioxidant, anti-inflammatory, and chemopreventive properties as well.[16]
The literature has shown conflicting results as to whether or not green tea has an effect on BC.[20,21] Yu et al. conducted a meta-analysis in 2019 that included 14 case–control studies. The study concluded that green tea may have reduced the incidence of BC among women who drink it on a regular basis.[22] The present study has demonstrated a different conclusion. No associations were observed between green tea and BC risk when the risk was not stratified based on the menstrual status; however, it showed a statistically significant risk increase among postmenopausal women.
Asian women tend to consume soy products much more than women in Western countries, and, in fact, reports indicate a lower incidence of BC among Asian women compared to their Western counterparts.[4] Moreover, Asian women who migrated to Western countries have a higher incidence rate of BC in the past few generations. Thus, the role of genetics is relatively small.[10] This led to a wide exploration of the high intake of soy isoflavones in the Asian diet as a possible factor in BC risk reduction. Multiple reports have determined the potential of soy isoflavones on BC risk as a protective supplement despite the different methodologies used.[22-25] First, the Singapore Chinese Health Study showed an 18% risk reduction of BC among those who consumed high amounts of soy isoflavones.[26] Second, a recent Chinese study including 300,000 women indicated that consuming high amounts of soy isoflavones is associated with risk reduction.[27] Moreover, the latest report, a meta-analysis published in 2022, concluded that women who consumed high amounts of soy isoflavones were at a lower risk of BC compared to those who did not.[28] Even though the proposed amount that leads to a significant risk reduction is not generally agreed on, it has been suggested that consumption of 75 mg/day of soy products is the optimal amount to achieve maximum protection.[29] In addition, early-life intake of isoflavone supplements is important and may reduce the risk of BC in adulthood.[29] Our study illustrates the potential role of adult intake in BC prevention, as soy milk has shown a significant risk reduction among Saudi women as a protective supplement against BC.
Flaxseed is a supplement rich in lignan, 100 times higher than other supplements.[30] Furthermore, chamomile is another medicinal plant that has antioxidant, anti-inflammatory, anticancer, and anti-microbial effects.[31,32] Studies have shown that consumption of both supplements can slow and prevent BC progression.[33-35] The anti-cancer effect of chamomile in BC patients could be due to apigenin, which inhibits cell proliferation and causes apoptosis and cell cycle arrest.[36,37] Nevertheless, the current study did not find an association even when the risk was stratified based on the menstrual status.
Some limitations should be considered before generalizing our findings. First, this is a case–control study, and there could be confounding bias in the estimation of the risk of BC due to potential confounders. However, we tried to reduce this bias by controlling for many factors, and the difficulty of including many other variables should be considered. Second, the supplement intake was recorded based on self-reported responses, which could have resulted in recall bias and social desirability bias. Third, other than those supplements, we did not record the usual diet of the participant, which could have distorted the risk estimation. Future research should fill in these gaps and follow a longitudinal study design that should involve a much larger sample of women taking supplements in a concurrent, sequential, and consistent manner.
Conclusion
Soy isoflavones continue to show a significant risk reduction that could be used for a modified approach to reduce the risk of BC. However, Echinacea, licorice root, and green tea have been shown to increase the risk of BC. Further longitudinal analytical studies are warranted to replicate and confirm the relationships of PSs with BC risk.
Ethical Approval and Consent of Participants
The study was conducted after approval of the ethics committee at the participating hospitals. Informed verbal consent was obtained from the participants before participation.
Competing Interests
The authors declare that there are no conflicts of interest. All authors reviewed and approved the final version of the manuscript.
Funding
This project was supported by the Deanship of Scientific Research at Taif University.
Author’s Contributions
Sahar Alnefaie: Conceptualization, literature review, study design, data collection, statistical analysis, and manuscript editing. Nawaf Alwagdani: Conceptualization, literature review, study design, data collection, statistical analysis, and manuscript writing. Rashed Althobaiti: Data collection, data interpretation, and manuscript writing. Khaled Almansori: Data collection, data interpretation, and manuscript writing. Yousef Alalawi: Data collection and manuscript editing. Eyad Al-Kharashi: Data collection and manuscript editing. Ahmed Al-Ameer: Data collection and manuscript editing. Maha Abdel Hadi: Data collection and manuscript editing.
Acknowledgment
The researchers would like to acknowledge the deanship of scientific research at Taif University for funding this work and, to thank those who actively participated in the data collection, namely, Abeer Alsulaimani, Ali Alghamdi, Amani Alrumaym, Balsam Alfaar, Basma Ghareeb, Goharah Alunizi, Ibtihal Alali, Mohamad Alluheed, Omer Alshahrani, Omnia Shaban, Reuof Alamri, Saad Alqarni, Wejdan Alatawi, and Zohoor Alhossaini.
References
- Global cancer statistics 2018:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424.
- [Google Scholar]
- Possible role of phytoestrogens in breast cancer via GPER-1/GPR30 signaling. Clin Sci (Lond). 2018;132:2583-98.
- [Google Scholar]
- Breast cancer risk in relation to urinary and serum biomarkers of phytoestrogen exposure in the European Prospective into Cancer-Norfolk cohort study. Breast Cancer Res. 2008;10:R32.
- [Google Scholar]
- Estrogenic activities of ten medicinal herbs from the Middle East. J Chromatogr Sci. 2013;51:33-9.
- [Google Scholar]
- Effects of phytoestrogens on the activity and growth of primary breast cancer cells ex vivo. J Obstet Gynaecol Res. 2019;45:1352-62.
- [Google Scholar]
- Soy, red clover, and isoflavones and breast cancer:A systematic review. PLoS One. 2013;8:e81968.
- [Google Scholar]
- Molecular mechanisms of anticancer effects of phytoestrogens in breast cancer. Curr Protein Pept Sci. 2018;19:323-32.
- [Google Scholar]
- Plasma phytoestrogens and subsequent breast cancer risk. J Clin Oncol. 2007;25:648-55.
- [Google Scholar]
- The prevalence extent of Complementary and Alternative Medicine (CAM) use among Saudis. Saudi Pharm J. 2017;25:306-18.
- [Google Scholar]
- Medicinal herbs used in traditional management of breast cancer:Mechanisms of action. Medicines (Basel). 2020;7:47.
- [Google Scholar]
- Echinacoside inhibits breast cancer cells by suppressing the Wnt/b-catenin signaling pathway. Biochem Biophys Res Commun. 2020;526:170-5.
- [Google Scholar]
- The anti-prolific effect of Echinacea pallida on BT-549 cancer cell line. Cancer Res. 2004;45:1010.
- [Google Scholar]
- Evaluation of estrogenic activity of licorice species in comparison with hops used in botanicals for menopausal symptoms. PLoS One. 2013;8:e67947.
- [Google Scholar]
- Estrogenic and antiproliferative activities of isoliquiritigenin in MCF7 breast cancer cells. J Steroid Biochem Mol Biol. 2002;82:315-22.
- [Google Scholar]
- Isoliquiritigenin induces growth inhibition and apoptosis through downregulating arachidonic acid metabolic network and the deactivation of PI3K/Akt in human breast cancer. Toxicol Appl Pharmacol. 2013;272:37-48.
- [Google Scholar]
- Dietary compound isoliquiritigenin, an antioxidant from licorice, suppresses triple-negative breast tumor growth via apoptotic death program activation in cell and xenograft animal models. Antioxidants (Basel). 2020;9:228.
- [Google Scholar]
- Green tea compounds in breast cancer prevention and treatment. World J Clin Oncol. 2014;5:520-8.
- [Google Scholar]
- Green tea consumption and risk of breast cancer:A systematic review and updated meta-analysis of case-control studies. Medicine (Baltimore). 2019;98:e16147.
- [Google Scholar]
- Use of isoflavone supplements is associated with reduced postmenopausal breast cancer risk. Int J Cancer. 2013;132:1439-50.
- [Google Scholar]
- Soy isoflavones consumption and risk of breast cancer incidence or recurrence:A meta-analysis of prospective studies. Breast Cancer Res Treat. 2011;125:315-23.
- [Google Scholar]
- Effect of dietary soy intake on breast cancer risk according to menopause and hormone receptor status. Eur J Clin Nutr. 2010;64:924-32.
- [Google Scholar]
- Soy intake and breast cancer risk in Singapore Chinese Health Study. Br J Cancer. 2008;99:196-200.
- [Google Scholar]
- Soy intake and breast cancer risk:A prospective study of 300,000 Chinese women and a dose-response meta-analysis. Eur J Epidemiol. 2020;35:567-78.
- [Google Scholar]
- Estimated Asian adult soy protein and isoflavone intakes. Nutr Cancer. 2006;55:1-12.
- [Google Scholar]
- Apilot study comparing the effect of flaxseed, aromatase inhibitor, and the combination on breast tumor biomarkers. Nutr Cancer. 2014;66:566-75.
- [Google Scholar]
- Apigenin and cancer chemoprevention:Progress, potential and promise (review) Int J Oncol. 2007;30:233-45.
- [Google Scholar]
- Antioxidant and anticancer activities of chamomile (Matricaria recutita L.) BMC Res Notes. 2019;12:3.
- [Google Scholar]
- Flaxseed and its lignan and oil components:Can they play a role in reducing the risk of and improving the treatment of breast cancer? Appl Physiol Nutr Metab. 2014;39:663-78.
- [Google Scholar]
- Exposure of breast cancer cells to a subcytotoxic dose of apigenin causes growth inhibition, oxidative stress, and hypophosphorylation of Akt. Exp Mol Pathol. 2014;97:211-7.
- [Google Scholar]
- Hepatoprotective effect of Matricaria chamomilla aqueous extract against 1,2-Dimethylhydrazine-induced carcinogenic hepatic damage in mice. Heliyon. 2020;6:e04082.
- [Google Scholar]
- Apigenin in cancer therapy:Anti-cancer effects and mechanisms of action. Cell Biosci. 2017;7:50.
- [Google Scholar]
- Induction of caspase-dependent extrinsic apoptosis by apigenin through inhibition of signal transducer and activator of transcription 3 (STAT3) signalling in HER2-overexpressing BT-474 breast cancer cells. Biosci Rep. 2015;35:e00276.
- [Google Scholar]




