
Three dimensional analysis of ground reaction force during level walking correlates with sacrum displacement
Address for correspondence: Aisha Farhana, Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, Jouf University, Sakaka, Aljouf, Saudi Arabia. E-mail: afarhana@ju.edu.sa
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Qassim Uninversity and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective:
We determined the association between sacrum displacement and ground reaction force (GRF) during walking on a level surface and identify the sub-phase of gait cycle most affected by GRF. The kinematic parameters of angular displacement of sacrum bone in three directions were measured and a correlation was derived to integrate the effect of GRF to sacrum displacement. Furthermore, gender variation in the sacrum bone configuration that induces the GRF to shift in one direction was determined.
Methods:
Forty healthy university students were evaluated for a normal gait pattern using the Qualysys motion capture system or a motion analysis system (MAS). The synchronization between MAS and force plate was done through computer software for the three-dimensional analysis (3D) of the force and angular displacement.
Results:
A positive correlation in the vertical direction was observed in the early and late phases of the stance phase in females. In males, a positive correlation was demonstrated in the middle and late phase of the stance phase. However, a positive correlation in the anteroposterior direction during the middle part of the stance phase was found only among the male group.
Conclusion:
Incorporation of strength training exercises help to increase the rotator muscle strength of the trunk and lower extremities in both genders. In the male group, flexors and extensors of the trunk and lower extremities in the middle part need to be focused during strength training, especially for athletes. This would be useful in decreasing the incidence of sports injuries.
Keywords
Athletes
gender difference
ground reaction force
level walking
sacrum displacement three-dimensional forces

Introduction
The human spine is a complex column that provides significant structural support with constrained motion located through its 24 articulating vertebrae. The morphological composition of the spinal cord is facilitated for the load-bearing capability of the vertebral segments, especially the sacrum.[1] As compared to the primates, who pose with only an intermittent upright gait, the human sacrum incorporates more bone segments into its fused mass with a wider sacral ala to support the increased axial load during prolonged upright ambulation and stance. Given that the sacrum is larger than the other spinal segments, its name is derived from the Latin and Greek roots of “os” sacrum, which means sacred bone and translates from the Greek hieron, osteon.[2]
The contribution of opposing forces on female pelvis facilitates to temporality broaden the pelvic region during childbirth. This phenomenon is only associated with the female gender and hence is an example of gender variation.[3] The sacrum, which is the key of the human skeletal system, links the spine to the iliac bones and remains crucial for hip stability.[4] Sexual dimorphisms in the sacrum are often the fundamental characteristics that determine sex differences in the skeleton of an individual in general and the pelvis in particular. The female sacrum is a smaller bone with a more triangular shape than its male counterpart. In both sacra, load transmissions are mainly concentrated in the upper parts of the sacral corpus. The male sacrum, in contrast, has larger overall dimensions and possesses broader lower segments than those of women designed to support more weight above them than the women.[5]
With regard to the ilium, the sacrum has six degrees of freedom of motion. In comparison to women, men often have a longer, narrower pelvis, and a more conical pelvic cavity.[6] These sex differences are also reflected in the biomechanics of the joint, and compared to the male sacroiliac joint (SIJ), the female SIJ is more mobile and experiences more stresses, loads, and strains in the pelvis and ligaments.[7]
The fundamental objective of walking is to move the body’s center of mass (COM) from one position to another. A periodic vertical displacement of COM, moving through a full cycle of vertical motion with each step, or through two cycles with each stride characterizes the normal human gait pattern. For adult ambulators at their freely chosen walking speed, the peak-to-peak amplitude of the vertical COM displacement, also known as the vertical excursion, is often estimated to be 4–5 cm. The center of gravity crosses each leg in the stance phase while moving side to side once in the frontal plane during a gait cycle. In addition, during the sagittal movement, the overall range is 4–5 cm.[8] The vertical COM motion during walking has been used to estimate mechanical energy changes to gauge efficiency, estimate work, describe symmetry, and as an indicator of the overall quality of gait.[9]
The results of our study coincide with that of Junggil et al., wherein they proved a three-dimensional correlation (vertical, medial, and anteroposterior) between the estimated ground reaction force (GRF) and the force plate measured GRF, in the midstance phase.[10] In the study, the participants used shoes with three uniaxial load cells using long-and short-term goal memory. Distinct results were obtained in the training set and the validation set compared to the test set.
Moreover, Dongwei et al. studied the correlation between the kinetic and kinematic data obtained from motion analysis system (MAS) during ascending and descending the stairs.[11] The study demonstrates a moderate correlation between anteroposterior and vertical directions and hip accelerations, body mass, and types of locomotion during both ascending and descending gait.
In addition, Ryota et al. designed two kinematic models of finite element method with and without SIJ.[12] They studied the load transition during five subphase of the gait cycle, concluding that a wide displacement of SIJ with the pelvic bone caused greater increase in the stress around the SIJ. Compared to the model without SIJ, a less concentration in the stress and little displacement was observed. Any musculoskeletal disorder of the hip joint, especially in infants, could directly affect the sacrum bone displacement. Therefore, it is extremely important that ultrasonography and clinical examination should be performed for the detection of onset of the developmental dysplasia of the hip in infants younger than 6 months.[13]
The objective of the present study is to determine if a correlation exists between the GRF and the sacrum displacement in the three directions. At present, there are no accurate studies in young males and females focusing on the forces that act on the sacral vertebra. In our study, we determine if the gender-biased structural configuration of the sacrum bone affects the force acting on the muscles around the pelvis and hip joint, and lower back beside the muscles of the lower extremities. Our study provides insights into the possible mechanisms that may be employed to decrease the incidence of back and pelvis injuries in both genders in an early age.
Materials and Methods
Study participants
The study was conducted at the Biomechanical Laboratory at the Faculty of Physical Therapy, Cairo University to assess the correlation between GRF and sacrum displacement in male and female students during walking on level surfaces. A three-dimensional analysis was done to evaluate the GRF. Forty healthy university students volunteered to participate in this study. All participants met the criteria that include an age ranging from 19 to 22 years old, and body mass index (BMI) of 20–25 kg/m2. All participants were free from any musculoskeletal problems. Participants with systemic or neurological diseases and musculoskeletal disease were excluded from the study. In addition, any abnormality in the pelvis or sacrum region especially a history of fracture that can affect pelvis inclination was considered as the exclusion criteria.
Power analysis was carried out using statistical software (G*Power v3.1.9.4, Düsseldorf, Germany). Mean and the difference were used to determine the sample size. As there were two independent groups with two mean selections, the t-test was applied. Effect size (d) was estimated from the literature between female and male groups.[14,15] The sample size of 40 including 20 males and 20 females has the mean age as 20.1 ± (1.34) years, mean body weight was 73.9 ± (11.34) kg, and mean height was 179.8 ± (12.69) cm. The study was authorized by the ethical committee board of the Faculty of Physical Therapy, Cairo University (Approval No. P.T.REC/012/004101). Before the followed experimental procedures, all participants gave their written consent.
Procedures
Qualysys motion capture system (mocap) preparations
mocap or a MAS was used in the present study in combination with a force plate component to extract the kinematic and kinetic data. The system structure comprised 6 high-velocity infrared Pro-Reflex cameras and an (Advanced Mechanical Technology Inc., USA [AMTI]) force plate placed in the center of a walkway. In this system, the force exerted by the human body on the plate is analyzed. The overall width of the mocap is 40 cm and its length is 60 cm. The sampling rate of the plate is 120 Hz. It includes four-strain gauge transducers organized at the corners of the plate. A long cable connects the force plate to a computer unit. The signals from the plate are amplified by an internal amplifier and fed through an analog to digital converter. The AMTI force plate uses a coordinate-oriented system to calculate GRF magnitude. This is attached to a computer software to capture the three-dimensional motion of the body parts, which is processed for each marker position, as Tab Separated Values [Figure 1].
- Tab Separated Values for gait cycle. (Abd-Eltawab et al. 2022). The figure depicts the three-dimensional data of each marker position obtained from the computer software and captured for the resultant data analysis. It represents a complete gait cycle from initial contact of the right leg to a successive initial ground contact of the same leg
In addition, the kinematic data were also obtained to determine the angular displacement of the sacrum bone while walking. A double-sided adhesive tape was used to attach the reflective markers to the skin at the recommended sites to obtain accurate kinematic data.
Each participant was asked to stand barefoot in front of the walkway and walk normally as much as possible without targeting on a slope during walking. Twenty reflective markers were located on body points.[16] These sites were: (1) Left and right shoulders, (2) sacrum, (3) the 12th thoracic vertebrae, (4) left and right greater trochanters, (5) left and right anterior superior iliac spines, (6) left and right suprapatellar regions, (7) left and right knee joint lines, (8) left and right tibial tuberosities, (9) left and right heels and toes (between the second and third metatarsals), and (10) left and right ankle joints. All the markers were applied to the skin using double-sided sticky tape. Before collecting the walking parameters, the Qualisys system was adjusted to focus each of the six cameras to pinpoint the locations of the reflecting markers in the walkway’s path field. Double-sided adhesive tape also facilitated all markers on the specific point landmarks. The validity and reliability of the Qualisys system were previously approved and were adjusted before picking up the required parameters, to enable each camera to determine the locations of the reflective markers.[17]
Statistical analysis
Correlation between various variables was calculated using Pearson’s moment correlation equation for linear relation of normally distributed variables. Spearman rank correlation equation was used for non-normal variables/non-linear monotonic relation. P < 0.05 was considered statistically significant. IBM SPSS (Statistical Package for the Social Science; IBM Corp, Armonk, NY, USA) release 22 for Microsoft Windows used for all statistical analyses. The data are normalized, with exclusion of any outliers. The normality and homogeneity of variance were tested statistically before using the parametric assumption.
Results
The assessment of GRF and sacrum displacement was conducted in the three dimensions X, Y and Z for both male and female groups. Three different sub-phases of gait cycle which are 0–20%, 20–30%, and from 30% to 60% were evaluated. A correlation between GRF and sacral displacement was carried out using Pearson’s moment correlation and Spearman rank correlation equations. Moreover, the three-dimensional kinematic analysis of the sacrum angular displacement in male and female groups during the whole gait cycle was also included. Table 1 demonstrates the demographic data comprising age and BMI of the subjects included in the study.

Male group correlation
The results of the present study showed a positive correlation between GRF and sacrum displacement at the sub-phase 20–30% (R = 0.633) in the X-direction. In addition, a positive correlation at the sub-phase 20–30% (R = 0.530) and a weak correlation at 30–60% (R = 0.485) in the Z-direction were observed. However, there was no significant correlation between GRF and sacrum displacement in the Y-direction [Table 2 and Figure 2a-c].
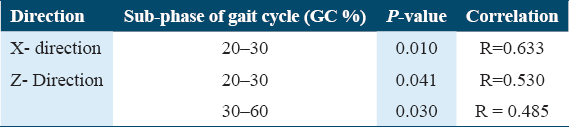
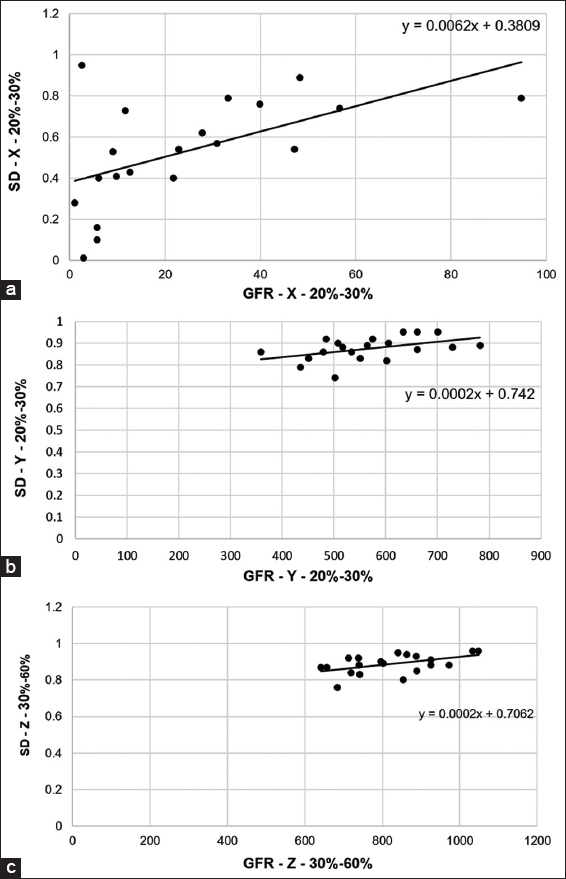
- Correlation between GFR and sacral displacement (SD) in the X-, Y-, and Z-direction among the males. Pearson’s correlation was used to calculate the level of correlation between GRF and SD. (a) The graph indicates a positive correlation between the two parameters (R = 0.633) in the X direction. (b) The graph indicates a positive correlation between the two parameters(R = 0.530) in Y direction. (c) The graph indicates a positive correlation between the two parameters (R = 0.485) in Z direction
Female group correlation
The results of this study revealed a positive correlation between GRF and sacrum displacement at the sub-phases 0–20 % (r = 0.539) and 30–60% in the Z-direction (R = 0.634). However, no correlation was found in either X or Y directions [Table 3, Figure 3a and b].

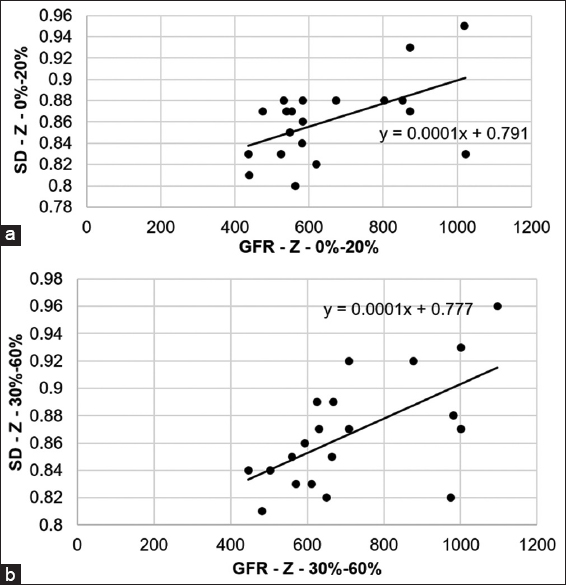
- Correlation between GFR and sacral displacement (SD) in the Z direction among females. The figure depicts a correlation between (a) GFR and SD from 0 to 20% angle ((r = 0.539) and (b) GRF and SD between 30 and 60% angle
The kinematic analysis of the sacrum angular displacement for male group in X-, Y-, and Z-directions
In X-direction
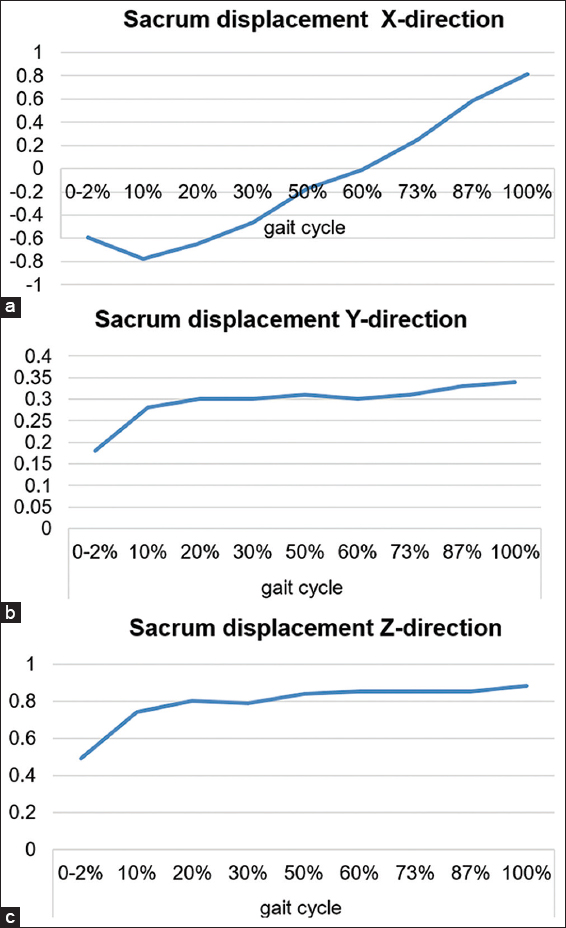
In Figure 4a, we observe an angular displacement of the sacrum for all sub-phases of the gait cycle from 0% up to 100% in males in X-direction during walking on level surface. There was a posterior displacement in male sacrum. This posterior displacement showed a decrease with increasing the percentage of the gait cycle from 0% nearly up to 50%. On the other hand, from 60% up to 100%, the posterior sacrum displacement showed an increase.
- Angular displacement of the sacrum in male group in X-, Y-, and Z-directions. (a) The graph indicates decrease in the posterior sacrum displacement with increasing the percentage of the gait cycle from 0% up to 50%. (a) The graph indicates medial displacement in the sacrum for all sub-phases of the gait cycle. (b) The graph indicates an upward trend and an increase in the sacrum displacement by increasing the percentage of the gait cycle
In Y-direction
As shown in Figure 4b, we observed a little variation in the sacrum displacement for male group in the Y-direction and a medial displacement in the sacrum for all sub-phases of the gait cycle.
In Z-direction
Figure 4c depicts that there was little variation in the sacrum angular displacement with a positive value, which increased by increasing the percentage of the gait cycle.
The kinematic analysis of the sacrum angular displacement for the female group in X-, Y-, and Z-directions
In X-direction
Figure 5a revealed a shift in the angular displacement of the female sacrum from posterior displacement in the first half of the gait cycle. In the second half of the gait cycle, the angular displacement shifted to anterior displacement. However, this displacement variation was within the normal limit.
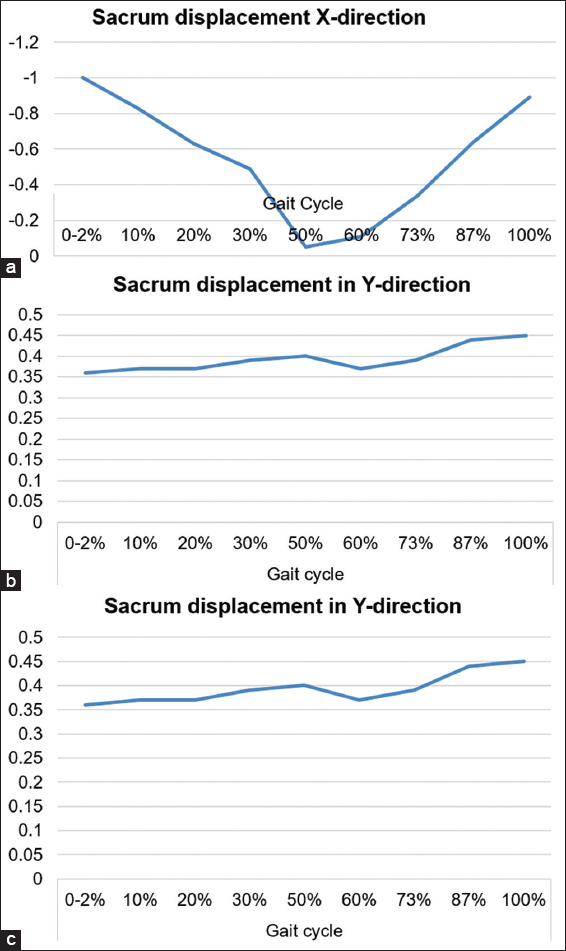
- Angular displacement of the sacrum in female group in X-, Y-, and Z-directions. (a) The graph shows shifting from the posterior to anterior sacrum displacement in the second part of gait in the X-direction. (b) The graph indicates medial displacement in the sacrum displacement in Y-direction, and (c) the displacement increases gradually within the limit with increasing the percentage of the gait cycle in Z-direction
In Y-direction
We observed a medial displacement in the sacrum displacement for the female group in the Y-direction present until the end of the stance phase [Figure 5b].
In Z-direction
According to Figure 5c, a vertical displacement exclusively in the positive direction for female sacrum displacement was noted. The displacement increases gradually within the limit with increasing the percentage of the gait cycle.
Discussion
The results of the present study illustrate a positive correlation between sacrum displacement and GRF in anteroposterior (X) and vertical directions (Z) for males and only in the vertical direction for females.[18] Hodges studied the force closure mechanism between the sacrum and the pelvis that is necessary for mobility. They revealed that if the sacrum fits in the pelvis in the form of closure, lateral compressional forces are not needed. However, with joint compression, both lateral force and friction are needed to withstand vertical load.[19]
The results of this study are in conjunction to our previous study, wherein we analyzed the three-dimensional direction (3D) of hip joint reaction force (JRF) using specialized AQHF software.[20] Different walking ramps were used to differentiate between gender mobility pattern with the value of GRF and JRF in the X-, Y-, and Z-directions. The study demonstrated that 3D hip JRF in males is higher than in females in all walking inclinations. Mixed Design MANOVA revealed significant differences between males and females among all tested inclinations in the study.[21]
The correlation that we observed in the present study in the vertical or anteroposterior direction may be attributed to gender differences in the sacrum bone. As noted by Gruss and Schmitt, the male sacrum is longer and flatter than the female sacrum and the female sacrum is wider and shorter.[22] The sacrum curves forward and terminates at the coccyx with a more protruded curvature in females than in males.[23] Accordingly, more load is required from the lower extremities, trunk, and pelvic muscles to oppose these forces on the sacrum bone. Wong et al. and Dolphens et al. also demonstrate that lower back discomfort has the sacrum as its main point. About 27% of all complaints of lower back discomfort may be attributed to forces placed on the sacrum and SIJ. Forward and backward tilting of the sacrum between the iliac bones impacts the joints between L5 and S1, thereby influencing the joints at the higher spinal levels. Sacral mobility involves the SIJ, which affects the discs and the upper lumbar joints. In addition, the erector spinae and gluteus maximus work together to govern the ilium and the sacrum in a functionally interdependent manner. Parts of the multifidi and erector spinae muscles join to the medial iliac crest and help to bring the sacrum into nutation. The gluteus maximus, which has connections to the sacral, draws the latter into the former.[24] In addition, Mahato proved that the female sacrum is associated with lumbosacral transitional vertebrae (LSTV) primarily in the form of L5–S1 accessory articulations.[17] Meanwhile, the male sacrum is related to sacralization of L5 more than any other variety of LSTV. This may result from a heavier male axial skeleton with more load, necessitating the entire fusion of the L5 vertebra to the sacral mass in the possible backdrop of a small five-segment sacrum. This is biomechanically undermorphed to optimize load transit from the sacrum toward the SIJ.[25]
The combination of more than one group of muscle to work in coherence to maintain and conserve balance is the basis of correlation as evident in our study. As reported by Arab et al., the latissimus and gluteus maximus muscles had a reciprocal relationship as opposed to the erector muscle, which only has one function.[28] The hamstrings are perfectly positioned to tilt the pelvis backward, especially in stooped positions and when sitting up straight. In addition, by pulling or contracting the biceps femoris and semimembranosus, the iliac bones are rotated posteriorly in relation to the sacrum. By pulling and dilating the composite layers, contraction of the multifidus and erector muscles would raise the tension across these composite layers of fascia, which would have the effect of dragging PSIS towards the midline and tightening the posterior part of the back muscle.[27]
Besides, this correlation in both directions in males compared to only one direction in females may be due to the difference in gender.[22] Cho et al. also studied morphology and metabolites important for inducing muscular contraction that could affect both males and females.[26] They showed that the compressive force produced by the male muscle while walking was dependent on muscle fiber distribution and mass of body cell for a greater reaction force of the lower limbs joint as compared to females.[28]
Regarding the three-dimensional kinematic analysis of the sacrum bone, it was revealed that there was no significant difference between males and females. It was reported by Sakaguchi et al. that no significant difference in the average of three-dimensional angular motions of the rear foot, knee, and hip joints for female and male runners during stance phase of running was present.[27] Thus, no significant difference in the three-dimensional angular displacement in the hip joint for male and female may reflect the same results for their sacrum according to the findings of the present study.
Gender comparison by Chung et al. revealed that female trunks showed five degree more extended posture in the sagittal plane during gait than male trunks, which attributed to lumbar lordosis.[28] During the swing phase of the gait cycle, the trunk motion appeared to counterbalance the lower extremity in the sagittal plane and to decrease the angular velocity toward the opposite side just before the opposite heel strike in the frontal plane. However, no significant kinematic sacrum angle analysis was mentioned in this study.[29,30]
Alcantara et al. evaluated the accuracy of sacral-mounted accelerometer data using quantile regression forest and linear regression models.[29] Their findings showed that over a range of running speeds, there were no significant differences connected to a single sacral-mounted accelerometer. Some studies assessed the kinematics of angular displacement of different joints during walking, running, and squatting for male and female genders.[22,27,28]
Some studies have also correlated the angular displacement of the sacrum in the three dimensions with the GRF in different phases of the gait cycle to be tested as a gender correlation value.[19,24] The correlation that was mentioned by Dongwei et al. proved that there is moderate correlation between GRF in vertical and anteroposterior directions and hip acceleration.[11] Thus, their results were in accordance with the results of our study as the sacrum bone is one of the anatomical configurations in the pelvic region that help in transferring body weight through the lower limbs.[3]
The connecting critical point regarding the type of rehabilitation program of the exercises in the three different planes of motions related to the selected type of exercise for both genders. As described by Paul et al., human movements occur in three dimensions based on a series of planes and axes.[30] Three planes of motion, namely, sagittal, frontal, and transverse planes pass through the human body.[31] Certain movement occurs in the anteroposterior direction (flexion-extension), mediolateral direction (abduction and adduction), and transverse or vertical direction (internal and external) rotation.[32] Another factor that may also contribute to the presence of positive correlation is inter-subject variation within the two gender groups. We previously reported that during level walking, males showed a considerably larger mass-specific mediolateral ground reaction than females. Both genders showed more inter-subject variation. Hence, a greater link between mediolateral GRF in females than in males between body weight and peak is present.[33-36] Therefore, concentrating on the muscles which perform various actions will help in improving the functional activities, especially for athletics to prevent sport-related injuries. In the present study, we have not assessed the psychological conditions of the participants and the functional variation among cases, which can potentially enhance the results of the present study. Furthermore, a better insight can be obtained using higher sample size for both genders and specialized software.
Conclusion
According to the present results, an increase in the sacrum displacement increases the value of GRF in the anteroposterior and vertical direction in the middle and late phase of the stance phase for male group. However, this increase occurs only in the vertical direction in the early and late part of the stance phase in female group. At present, there is a lack of studies related to each sub-phase that analyze the gait in three different directions to correlate with GRF. This study holds promise in understanding a correlation between sacral displacement and GRF focusing on the group of muscles to design a rehabilitation program for athletics with a similar age group as of the selected sample. The findings of the present study propose to increase the strength of rotators muscle of the trunk and lower extremities in both males and females and have also been reported previously.[29] The male group can benefit from strengthening the flexors and extensors of the trunk and lower extremities in the middle part of the stance phase (from 30% up to 60%), especially for athletic males to decrease the incidence of sport-related injuries.
Ethics Approval and Consent to Participate
The study was authorized by the ethical committee board of the Faculty of Physical Therapy, Cairo University (Approval No. P.T.REC/012/004101). Before the followed experimental procedures, all participants gave their written consent.
Author Contribution
AEA, AMA, and AF were responsible for composing the manuscript; AEA, and AMA were responsible for conceiving the experimental study design, performing the experiment, and statistical analysis; AF and HBG analyzed the data and edited the manuscript. All authors were involved in reviewing the manuscript. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
The authors deeply acknowledge the University for supporting various stages of this work.
Funding
This work did not receive funding from any organizations.
Conflicts of Interest
The authors declare no conflicts of interests.
References
- The American Heritage Dictionary of the English Language (4th ed). Boston: Houghton Mifflin; 2000.
- Basic Biomechanics (7th ed.). New York: McGraw-Hill Education; 2015.
- Sacrum and Lumbosacral Joints. In: Gray's Anatomy. (38th ed.). London, UK: Churchill Livingstone; 1995. p. :531-3.
- [Google Scholar]
- Clinically Oriented Anat (7th ed). Philadelphia, PA: Lippincott Williams and Wilkins; 2014.
- Sex specific sacroiliac joint biomechanics during standing upright:A finite element study. Spine (Phila Pa 1976). 2018;43:E1053-60.
- [Google Scholar]
- Anatomy and Human Movement:Structure and Function (6th ed). Edinburgh: Churchill Livingstone; 2012.
- Mechanical work for step-to-step transitions is a major determinant of the metabolic cost of human walking. J Exp Biol. 2002;205:3717-27.
- [Google Scholar]
- A deep learning model for 3D ground reaction force estimation using shoes with three uniaxial load cells. Sensors (Basel). 2023;23:3428.
- [Google Scholar]
- Deep learning based ground reaction force estimation for stair walking using kinematic data. Measurement. 2022;198:111-344.
- [Google Scholar]
- Finite element analysis of load transition on sacroiliac joint during bipedal walking. Sci Rep. 2020;10:13683.
- [Google Scholar]
- Developmental dysplasia of the hip in infants younger than six months:Ultrasonographic assessment in relation with risk factors. Int J Health Sci (Qassim). 2023;17:37-45.
- [Google Scholar]
- Explaining the hip adduction moment variability during gait:Implications for hip abductor strengthening. Clin Biomech (Bristol, Avon). 2009;24:267-73.
- [Google Scholar]
- Pelvic Shape, Hip Abductor Mechanics and Locomotor Energetics in Extinct Hominins and Modern Humans. St. Louis: Washington University; 2011.
- Percentage contribution of lower limb moments to vertical ground reaction force in normal gait. J Chiropr Med. 2019;18:90-6.
- [Google Scholar]
- Qualisys Track Manager User Manual. Gothenburg: Qualisys AB; 2006.
- Quantitative analysis of factors affecting intraoperative precision and stability of optoelectronic and electromagnetic tracking systems. Med Phys. 2002;29:905-12.
- [Google Scholar]
- Core stability exercise in chronic low back pain. Orthop Clin North Am. 2003;34:245-54.
- [Google Scholar]
- Three dimensional analysis of hip joint reaction force using Q Hip force (AQHF) software:Implication as a diagnostic tool. PLoS One. 2022;17:e0273159.
- [Google Scholar]
- The evolution of the human pelvis:Changing adaptations to bipedalism, obstetrics and thermoregulation. Philos Trans R Soc Lond B Biol Sci. 2015;370:20140063.
- [Google Scholar]
- Anatomy, abdomen and pelvis, sacroiliac joint. In: In:StatPearls. Treasure Island, FL: StatPearls Publishing; 2021.
- [Google Scholar]
- Multivariable modeling of factors associated with spinal pain in young adolescence. Eur Spine J. 2016;25:2809-21.
- [Google Scholar]
- Relationship of sacral articular surfaces and gender with occurrence of lumbosacral transitional vertebrae. Spine J. 2011;11:961-5.
- [Google Scholar]
- The relationship between hamstring length and gluteal muscle strength in individuals with sacroiliac joint dysfunction. J Man Manip Ther. 2011;19:5-10.
- [Google Scholar]
- Gender differences in three dimensional gait analysis data from 98 healthy Korean adults. Clin Biomech (Bristol, Avon). 2004;19:145-52.
- [Google Scholar]
- Gender differences in hip and ankle joint kinematics on knee abduction during running. Eur J Sport Sci. 2014;14(Suppl 1):S302-9.
- [Google Scholar]
- Kinematic aspects of trunk motion and gender effect in normal adults. J Neuroeng Rehabil. 2010;7:9.
- [Google Scholar]
- Sacral acceleration can predict whole-body kinetics and stride kinematics across running speeds. PeerJ. 2021;9:e11199.
- [Google Scholar]
- Three-dimensional CNT-rGO/PDMS porous scaffold derived supercompressible lightweight body-mounted piezoresistive force sensor for human motion monitoring. Colloids and Surfaces A:Physicochemical and Engineering Aspects 675 (2023):131993.
- [Google Scholar]
- Gray's Anatomy (41st ed.). Edinburgh: Elsevier Churchill Livingstone; 2016.
- Hip abductor function and lower extremity landing kinematics:Sex differences. J Athl Train. 2007;42:76-83.
- [Google Scholar]
- Three-Dimensional Analysis of Human Movement. Champaign, IL: Human Kinetics Publication; 1995.
- Sex differences in lower extremity biomechanics during single leg landings. Clin Biomech (Bristol, Avon). 2007;22:681-8.
- [Google Scholar]
- Public speaking performance improvement as a function of information processing in immediate and delayed feedback interventions. Commun Educ. 2009;49:365-74.
- [Google Scholar]
- Sexual dimorphism impact on the ground reaction force acting on the mediolateral direction during level walking:Hip Abductor muscle biomechanics and its correlation to GRF moment arm. Front Bioeng Biotechnol. 2022;10:863194.
- [Google Scholar]




